Microscopy Images
![Reddish-brown 2,8-DHA crystals in tubules and interstitium with interstitial inflammatory reaction (hematoxylin and eosin [H&E] stain).](../assets/28-Dihydroxyadeninuria_001.jpg)
Patients may present in childhood with recurrent nephrolithiasis, but two-thirds do not present until the fourth decade. Adult patients present most commonly with nephrolithiasis, but chronic kidney disease (CKD), and less often acute kidney injury, may be seen. Patients may also present with urinary tract infection. 2,8-Dihydroxyadenine (2,8-DHA) stones are radiolucent and may be misdiagnosed as uric acid stones. Patients may be misdiagnosed clinically as having oxalosis due to elevated oxalate blood levels, however, levels are lower than with primary hyperoxaluria. 2,8-DHA crystals can be seen in urine at physiologic pH. Kidney crystals and stones may recur in those receiving a kidney transplant. Prognosis is excellent with allopurinol therapy started before CKD ensues, resulting in soluble adenine instead of insoluble 2,8-DHA crystals.
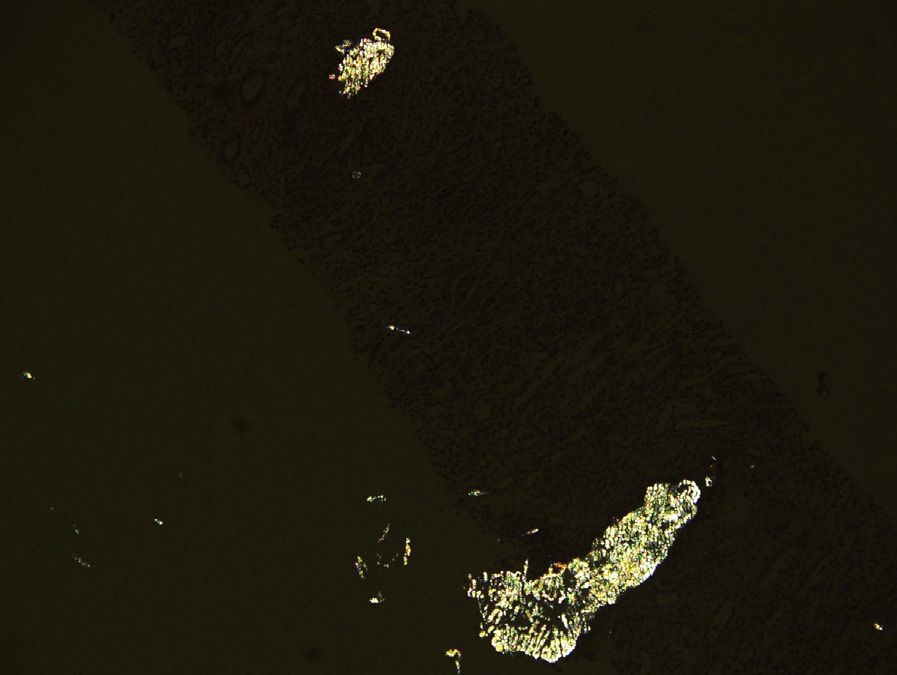
Light microscopy: Numerous 2,8-DHA crystals are present in tubular lumens, tubular epithelial cell cytoplasm, and interstitium. The crystals are reddishbrown on H&E and periodic acid–Schiff stains, black on silver stain, blue on trichrome stain, and birefringent under polarized light. Interstitial crystals cause an interstitial inflammatory reaction, including foreign body giant cells. Crystals can be found as single crystals or in aggregates with needle, rod, or rhomboid shape, and may be fan-shaped. Acute tubular injury is associated with crystals in the acute phase. Tubulointerstitial fibrosis occurs with chronic injury.
Immunofluorescence microscopy: Noncontributory.
Electron microscopy: Noncontributory.
2,8-DHA crystals occur secondary to genetic deficiency of adenine phosphoribosyltransferase (APRT), a purine salvage enzyme that converts adenine to adenosine monophosphate. In the absence of APRT, adenine is metabolized to 2,8-DHA by xanthine oxidase.
The resulting 2,8-DHA crystallizes in water. The inheritance is autosomal recessive, with complete deficiency in type I and limited residual enzyme activity in type II mutations. Type I is the most common form in those of European ancestry and type II is the most common in Japanese. In the former, the incidence of homozygosity is estimated to be 1 in 50,000 to 100,000.
Oxalate crystals are birefringent under polarized light, but are colorless by light microscopy.
Calcium phosphate crystals appear purple to blue on H&E-stained slides, and are not birefringent under polarized light.
Urate crystals are colorless and needle-like, and require alcohol fixation to be visualized by light microscopy.
These crystals dissolve by routine processing and are present as needle-like clefts crystals within the tubule, with tubular degeneration and surrounding inflammatory reaction and fibrosis.
Cystine crystals are colorless, rectangular, and refractile under polarized light and visualized in frozen material or after alcohol fixation, as they dissolve by routine processing.