Microscopy Images
Acute interstitial nephritis (AIN) describes a lesion with interstitial edema with a mononuclear cell infiltrate invading the interstitium and tubules, composed mostly of T lymphocytes. There are scattered plasma cells and macrophages, occasionally with non-necrotizing granulomas, and variable presence of eosinophils. When inflammation is due to infection, the lesion is diagnosed according to the specific pathogen involved (eg, bacterial, viral, or fungal). AIN commonly manifests clinically as acute kidney injury, with rapid decline in glomerular filtration rate, often with fever, eosinophilia, hematuria, sterile pyuria, and non-nephrotic proteinuria. In some cases with nonsteroidal anti-inflammatory drugs (NSAIDs)-induced AIN, there may be concurrent induction of minimal change disease–type injury, with nephrotic proteinuria. AIN occurs at any age. AIN may be recoverable if the underlying etiology is recognized and ongoing exposure is stopped.
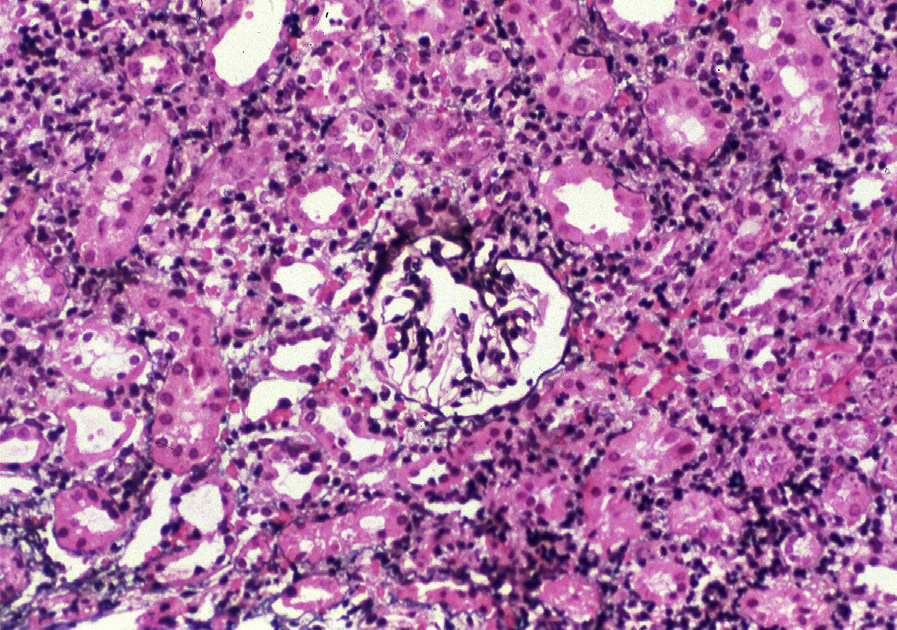
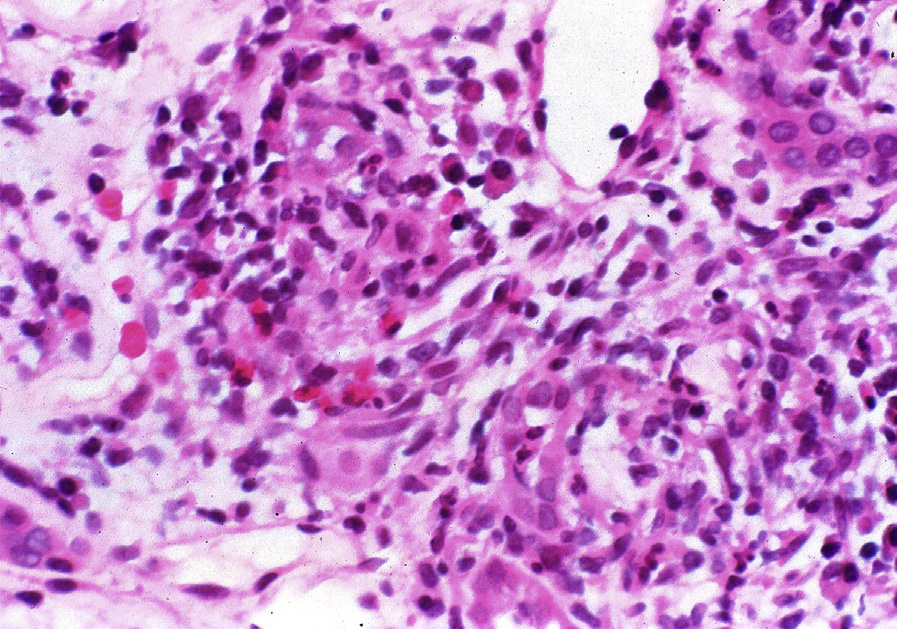
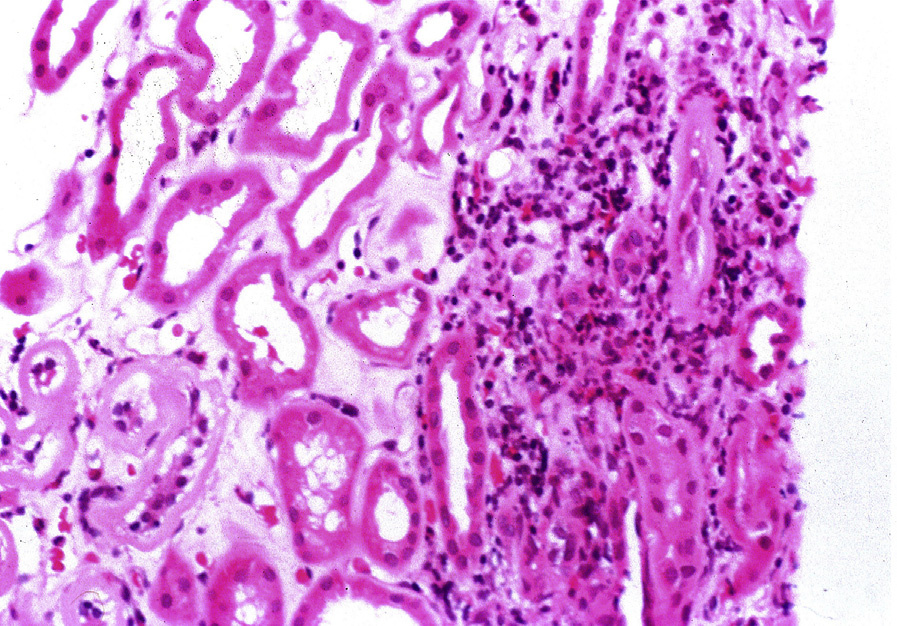
Light microscopy: There is patchy edema and mononuclear cell infiltrate, with mostly T lymphocytes, variable plasma cells, and macrophages. Tubulitis is typically present with concomitant variable acute tubular injury. There may be non-necrotizing granulomas, which are often ill-defined. Eosinophils are variably present.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: Typically there are no specific findings. In some cases with NSAIDs-induced AIN, there may be concurrent induction of minimal change disease–type injury, with extensive foot process effacement.
AIN is most often caused by allergic reaction to drugs or herbal remedies. Commonly implicated drugs include β-lactam antibiotics, NSAIDs, and proton pump inhibitors.
AIN may also occur secondary to anti–tubular basement membrane antibodies (diagnosed by linear tubular basement membrane staining with anti–immunoglobulin G), tubular basement membrane immune complexes (with granular tubular basement membrane staining on immunofluorescence microscopy), and infection with virus (specific inclusions), fungi, tuberculosis (may have necrotizing granulomas and organisms identified on stains or culture), or bacteria (numerous interstitial neutrophils, and neutrophil casts). Patients with acute tubulointerstitial nephritis with uveitis are diagnosed by clinical recognition of concurrent uveitis.
Necrotizing glomerulonephritis or vasculitis is commonly associated with active interstitial inflammation that, in limited samples with no glomeruli, may be mistaken as AIN. Non-necrotizing granulomas also occur with sarcoidosis, but are then often numerous, welldefined, and confluent.