Microscopy Images
Adenovirus renal infections usually occur in immunocompromised patients, more commonly in bone marrow and stem cell transplant recipients. Infections rarely (<1%) occur in the kidney allograft, with onset typically in the first 3 months after transplantation. Native kidney infections occasionally occur, mostly in children under 5 years of age. Patients usually present with fever, acute kidney failure, gross hematuria, and diarrhea. Kidney transplant patients can have tenderness over the graft.
Infection limited to the kidney transplant may respond well to decreased immunosuppression, with intravenous immunoglobulin and possible antiviral therapy suggested in more severe cases. Adenovirus can also infect the urinary bladder, lung, liver, and gastrointestinal tract.
Disseminated adenovirus in the immunocompromised patient is often (>60%) fatal.
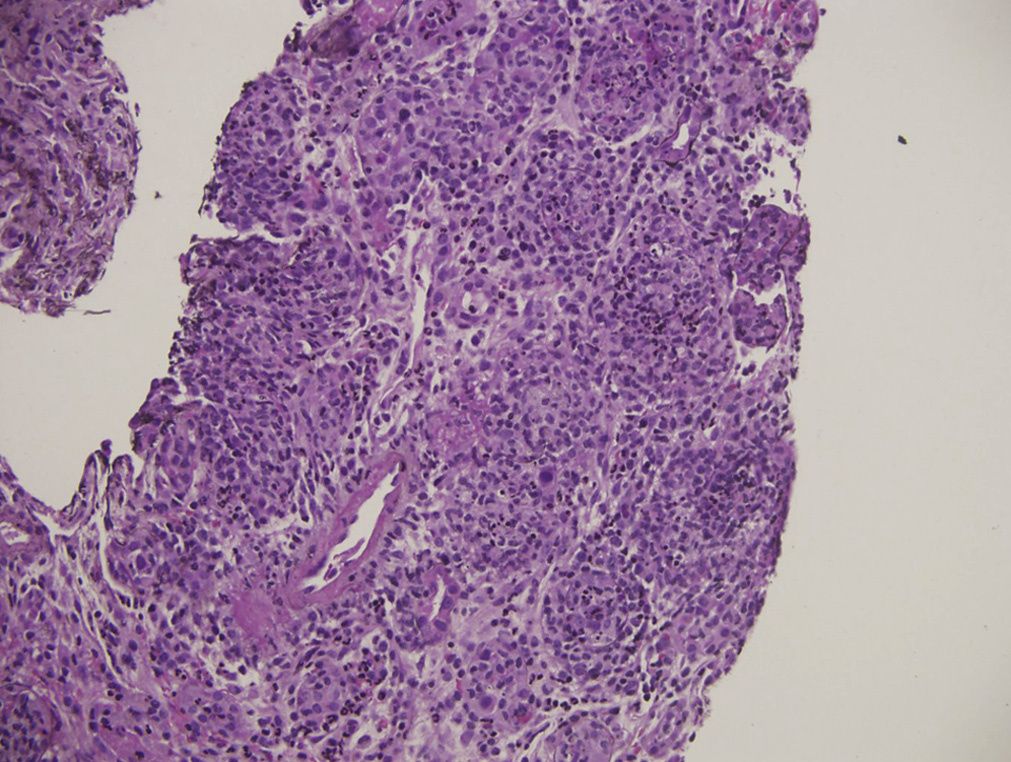
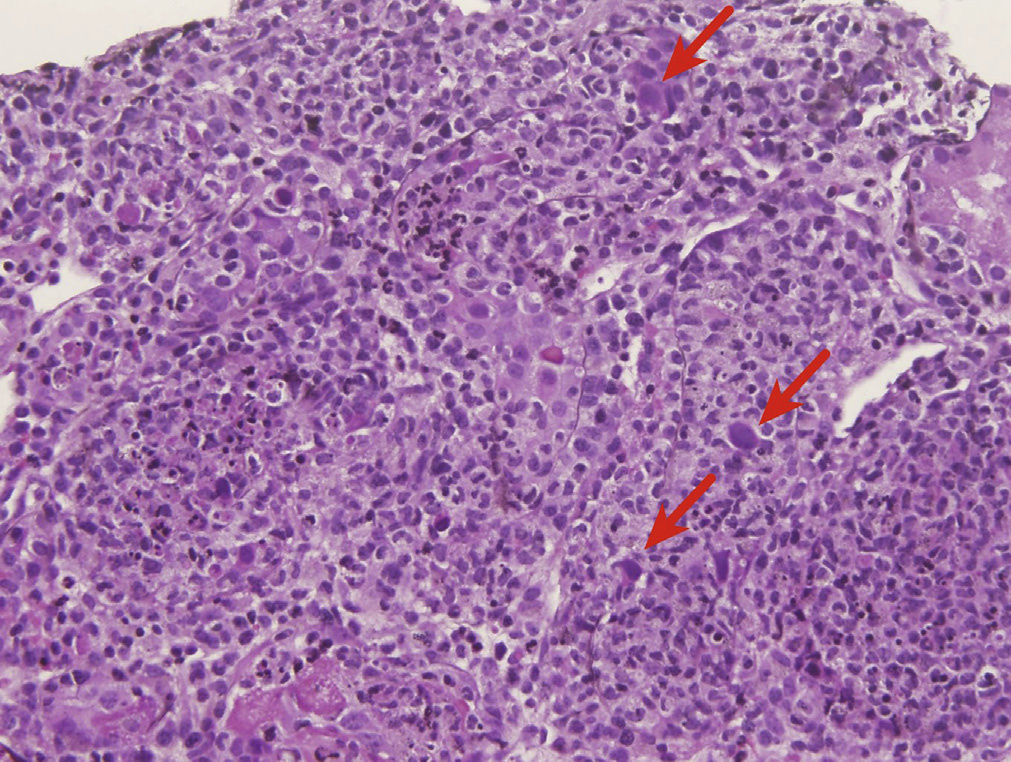
Light microscopy: Viral cytopathic changes consist of smudgy basophilic intranuclear inclusions with enlarged nuclei of infected cells. Distal tubules are more commonly involved than proximal tubules. Occasionally glomerular visceral and parietal epithelial cells can be infected. There is associated acute tubular injury, often with frank tubular necrosis and destruction, with acute interstitial nephritis, often with a pleomorphic infiltrate composed of lymphocytes, histiocytes, plasma cells, and variable numbers of neutrophils, with interstitial edema and hemorrhage.
Tubular destruction may be associated with necrotizing interstitial granulomas.
Severe granulomatous tubulointerstitial nephritis appears to be characteristic of adenoviral infection and is quite rare in other viral infections. Focal wedge-shaped necrosis may occur in renal parenchyma.
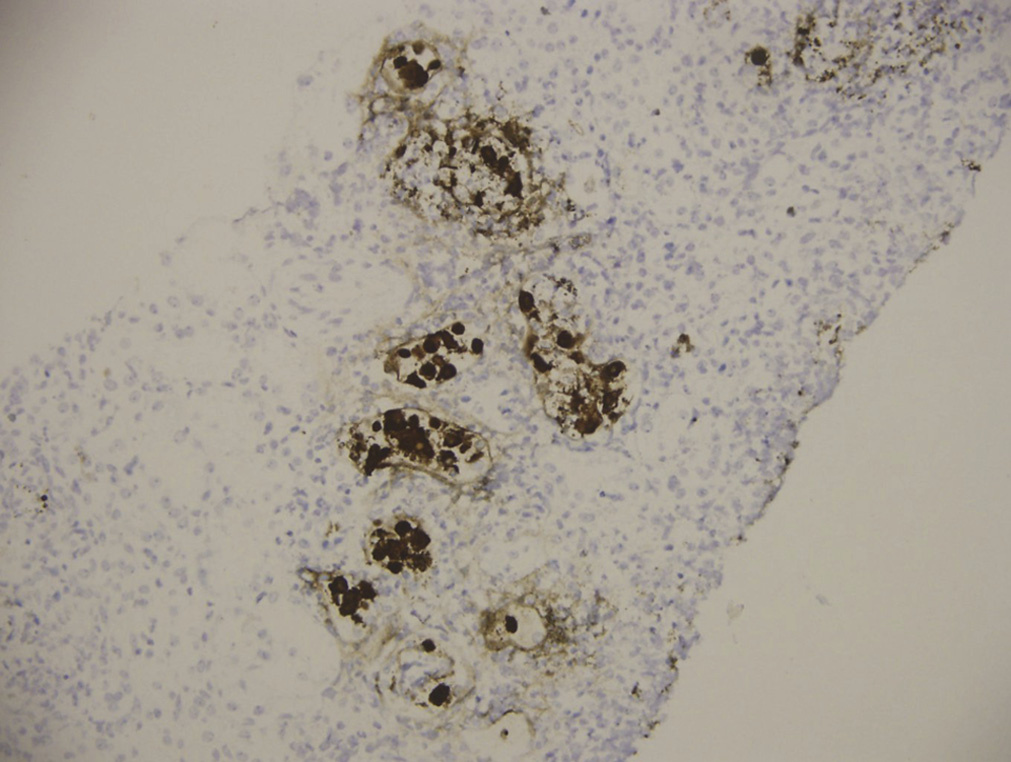
Immunostaining for adenovirus shows strong nuclear and cytoplasmic staining in infected cells.
Immunofluorescence microscopy: No specific staining.
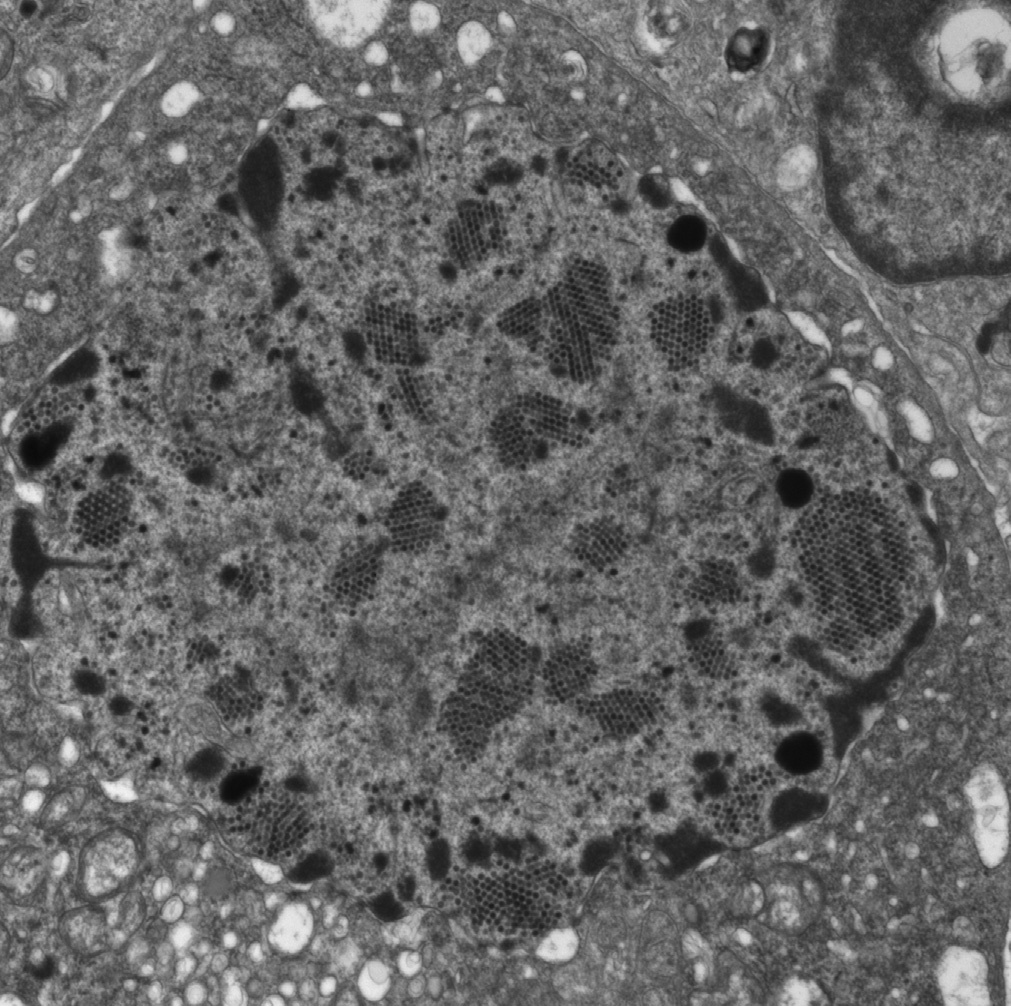
Electron microscopy: Viral particles are seen in infected epithelial nuclei and cytoplasm and are nonenveloped with hexagonal outline and a diameter of 70 to 110 nm, aggregated in a crystalline array.
Adenovirus is a nonenveloped, double-stranded DNA virus that is thought to infect the kidney through reactivation of latent infection in native or transplanted tissue.
Acute cellular rejection has a T cell–dominant interstitial infiltrate without viral cytopathic changes within tubular epithelial cells. The presence of vascular rejection with endothelialitis is diagnostic for T cell–mediated rejection, even in the presence of adenovirus infection confirmed by adenovirus immunostaining. Polyomavirus-related cytopathic changes can overlap with adenovirus-related cytopathic changes. Polyomavirus nephropathy usually has a more plasma cell–rich pleomorphic infiltrate without interstitial hemorrhage and infected tubular epithelial cell nuclei stain strongly for SV40. Granulomatous interstitial nephritis is very rare in polyomavirus nephropathy. Hantavirus infection can show a predominantly mononuclear cell interstitial infiltrate with interstitial hemorrhages associated with viral cytopathic changes without adenovirus immunostaining positivity.
Tuberculosis infection has multifocal necrotizing granulomatous interstitial nephritis with positive special stain for acid-fast bacilli. Acute pyelonephritis has a marked, predominantly neutrophilic interstitial infiltrate with neutrophil plugs within tubules without viral cytopathic changes. Acute interstitial nephritis due to drug-induced hypersensitivity reaction may have more frequent interstitial eosinophils without viral cytopathic changes and the absence of adenovirus immunostaining.