Microscopy Images
Chronic antibody-mediated rejection is commonly associated with progressive loss of kidney function and proteinuria, although early stages may be subclinical and recognizable only through protocol biopsies.
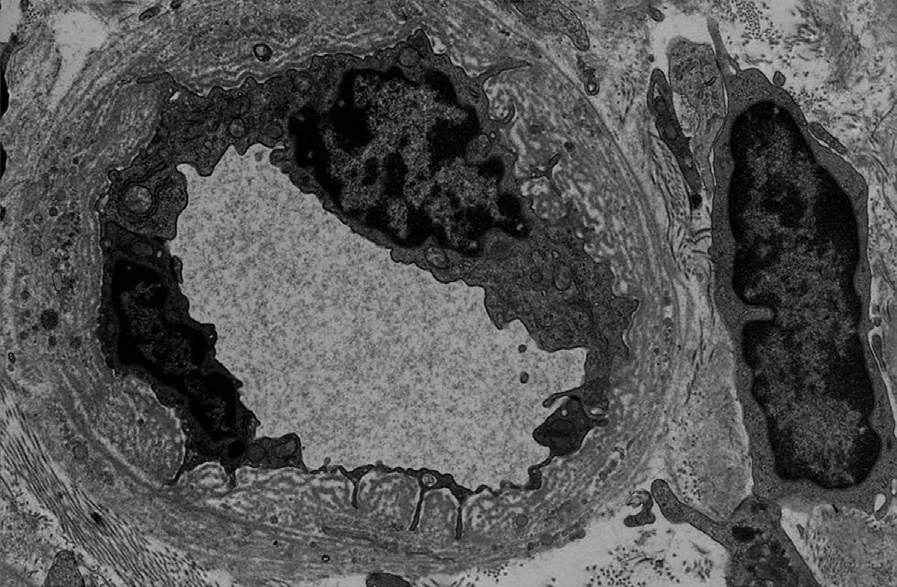
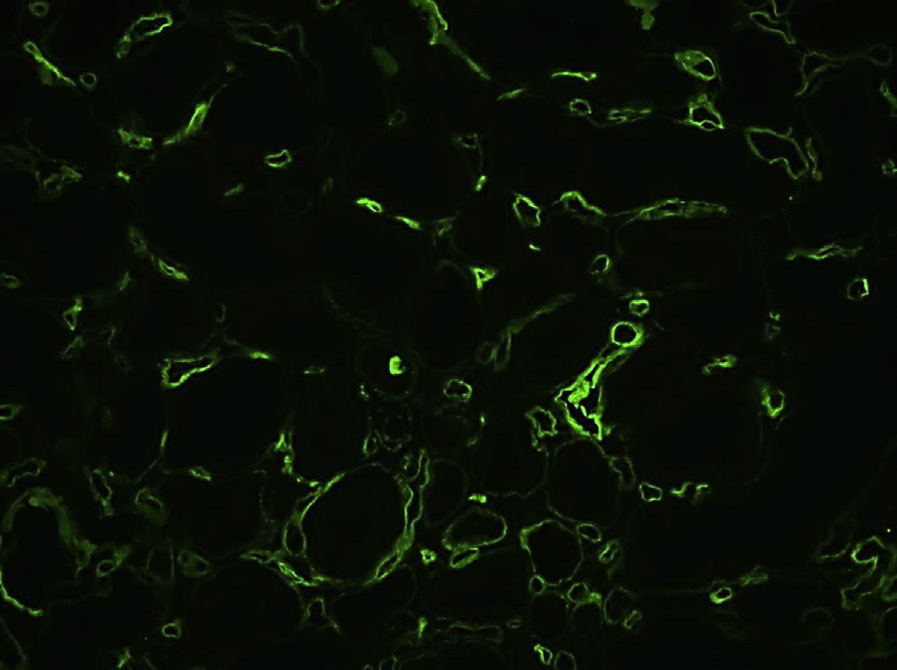
Diagnostic criteria according to the Banff 2013 classification (Haas et al, Am J Transplant 2014: 14(2):272-283) include the presence of all of the following: 1. Histologic evidence of chronic tissue injury, defined by the presence of at least one of the following: a. Transplant glomerulopathy (cg > 0) in the absence of chronic thrombotic microangiopathy b. Severe peritubular capillary basement membrane multilayering by electron microscopy c. New-onset arterial intimal fibrosis with no other known etiology 2. Current/recent histologic evidence of antibody interaction with vascular endothelium, defined by the presence of at least one of the following: a. Linear C4d staining in peritubular capillaries (at least 10% by immunofluorescence [IF] on frozen sections or any positivity by immunohistochemistry on paraffin sections) b. At least moderate microvascular inflammation (g + ptc ≥ 2) c. Increased expression of tissue gene transcripts indicative of endothelial injury 3. Presence of donor-specific antibodies (DSA; HLA or non-HLA) in the serum
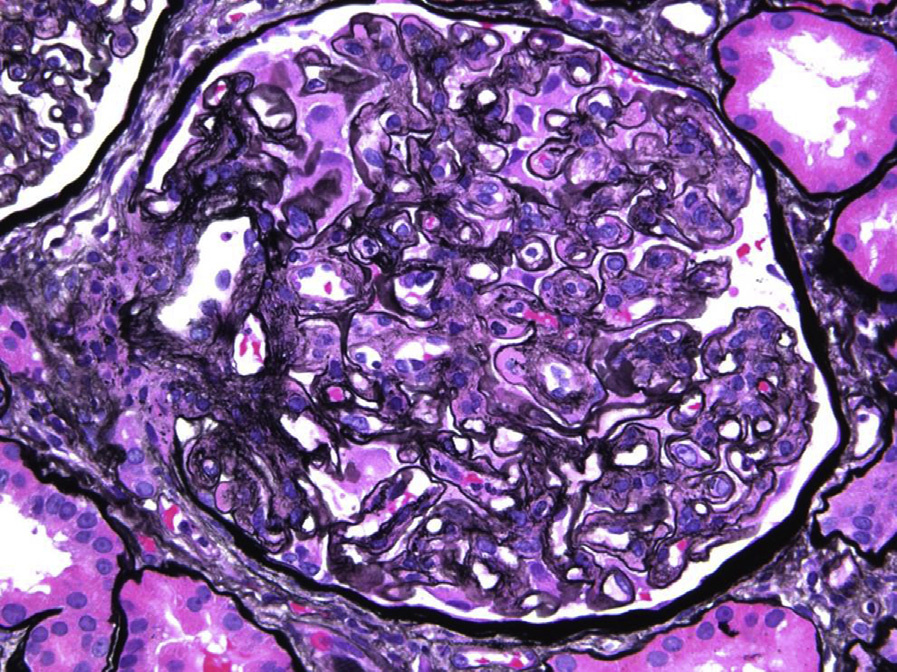
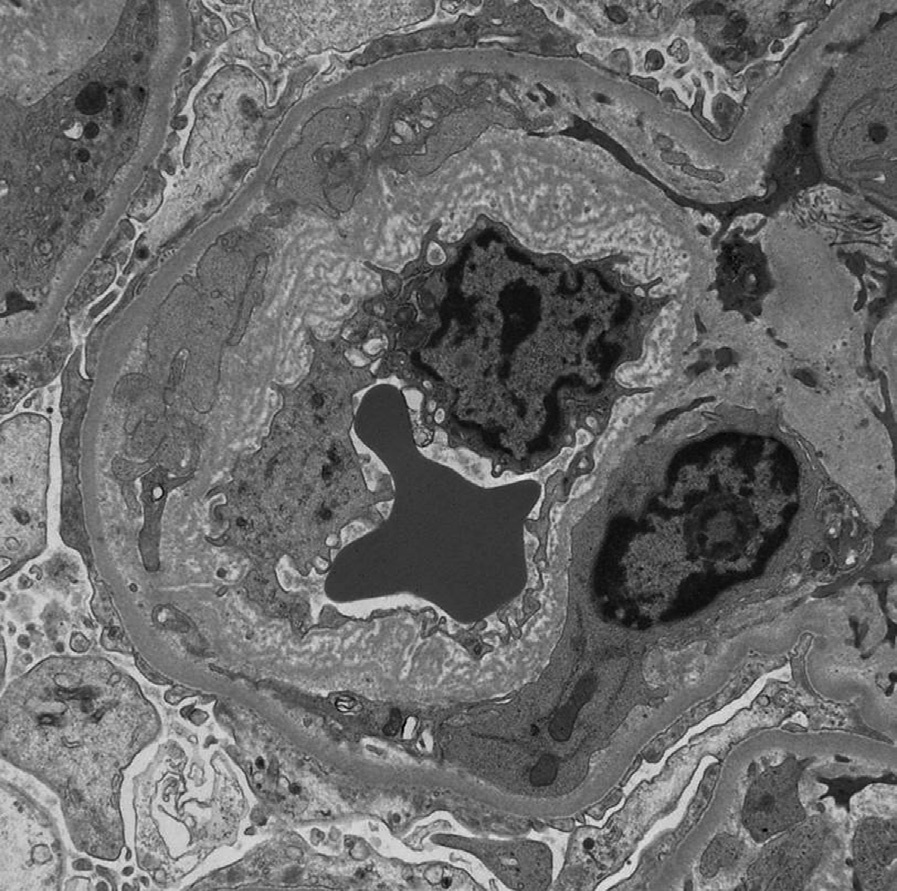
Similar to acute antibody-mediated rejection, endothelial injury results from interaction between DSA with primarily mismatched HLA or non-HLA molecules. Repetitive and chronic endothelial damage is associated with new basement membrane formation, which in glomeruli manifests as glomerular basement membrane duplication (transplant glomerulopathy), often with resulting segmental sclerosis, and multilayering of the peritubular capillary basement membrane. Podocyte injury and foot process effacement are common findings.
Glomerular basement membrane duplication is also found in other conditions associated with chronic endothelial damage, causing a membranoproliferative pattern of injury. Chronic thrombotic microangiopathy may be indistinguishable from transplant glomerulopathy on a morphologic basis unless features of concomitant acute thrombotic microangiopathy or vascular changes are present. In such cases, correlation with clinical history will be important. Membranoproliferative glomerulonephritis due to immune complex processes (lupus nephritis, immunoglobulin A nephropathy, cryoglobulinemic glomerulonephritis, etc) must be ruled out by IF and electron microscopy.
Peritubular capillary basement membrane multilayering, especially if not severe (,7 layers), is not specific to chronic antibody-mediated rejection.
Arterial intimal fibrosis is a common finding, often associated with chronic hypertension and aging.
Scattered T cells and foam cells may be present in the expanded intima, but are not specific for chronic antibody-mediated rejection and may also be seen in chronic T-cell–mediated rejection.