Microscopy Images
Acute antibody-mediated rejection is often asymptomatic, but more severe forms present with an acute drop in glomerular filtration rate, which may be accompanied by proteinuria.
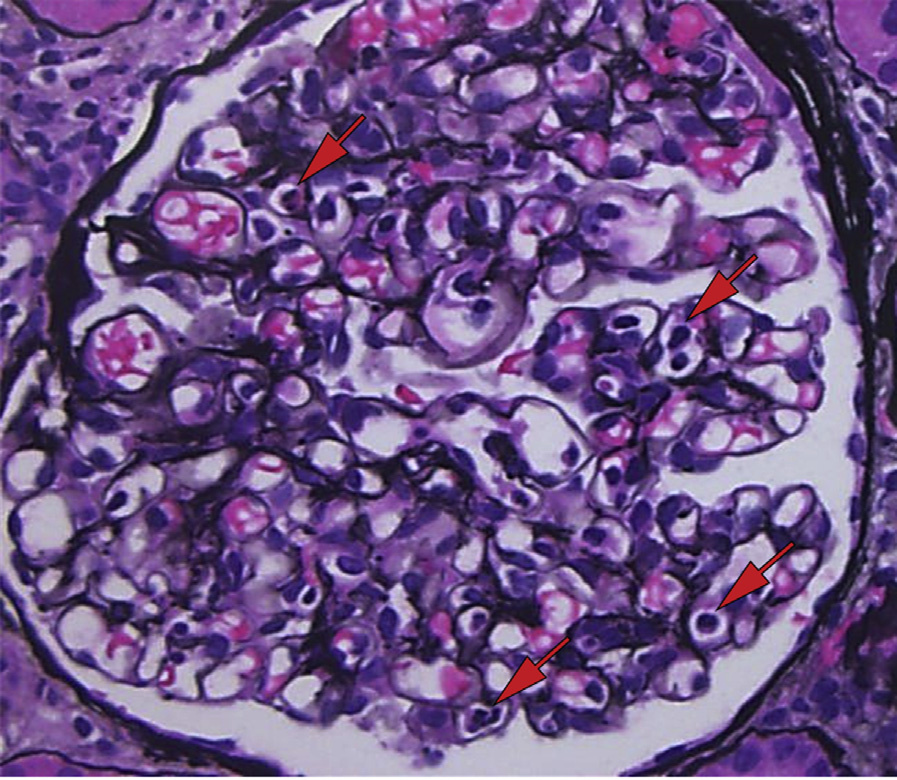
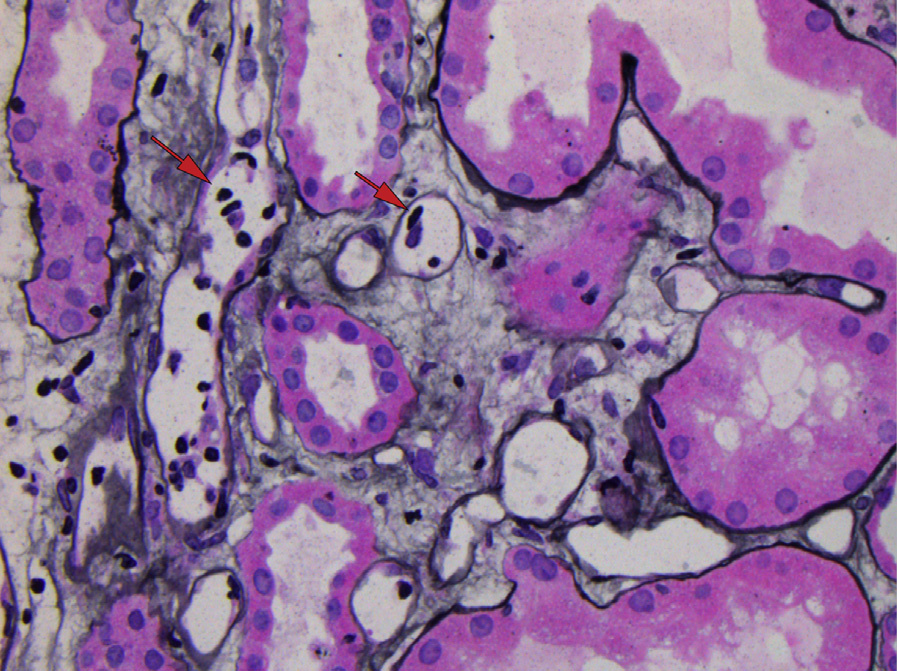
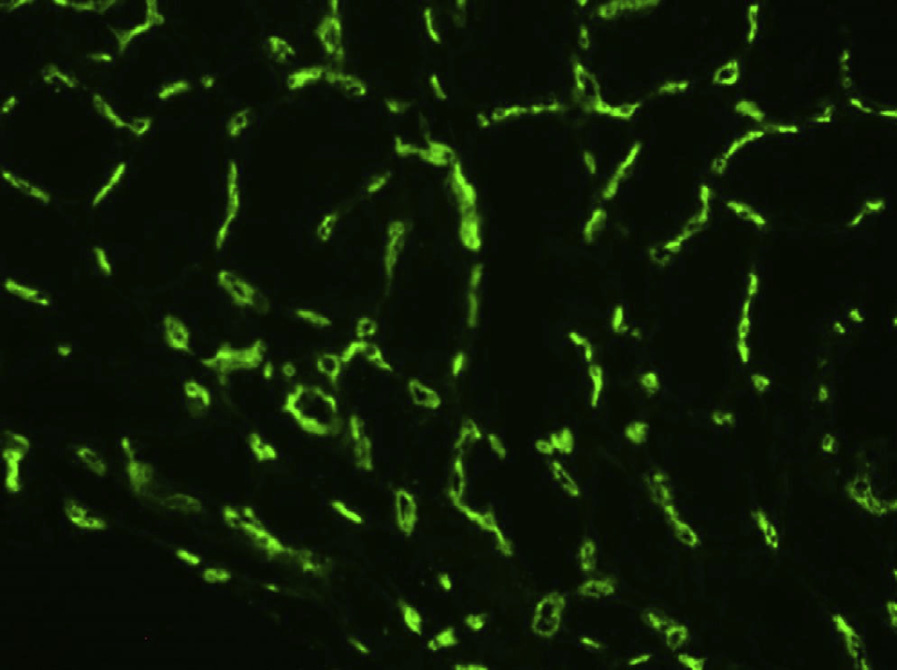
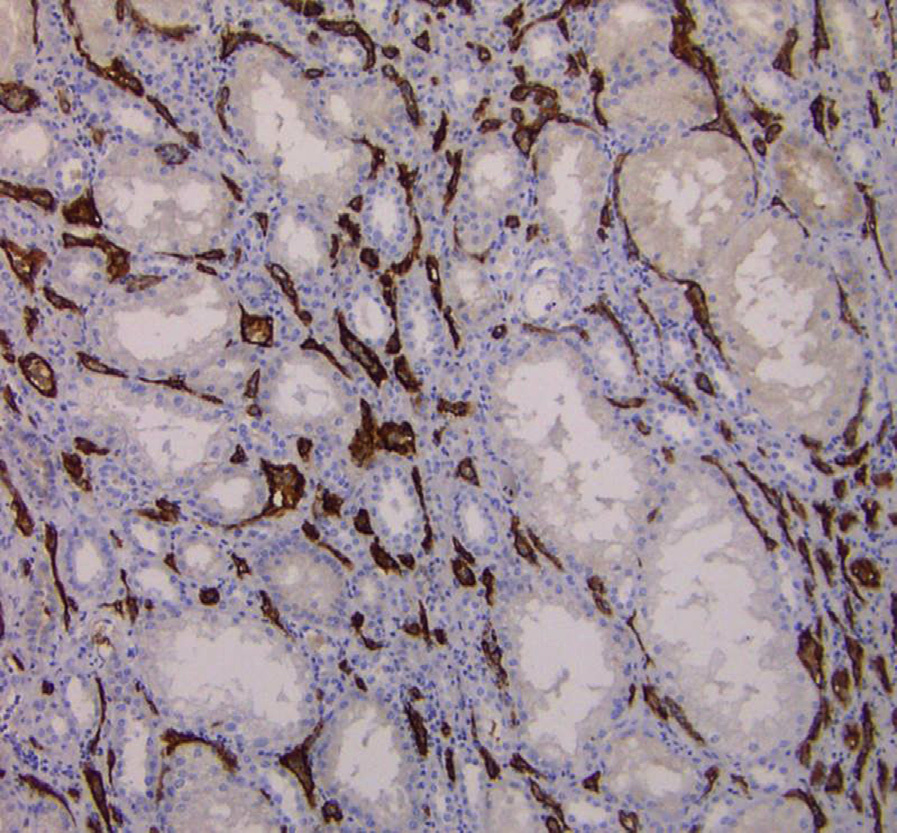
Diagnostic criteria according to the Banff 2013 classification (Haas et al, Am J Transplant 2014:14(2): 272-283) include the presence of all of the following: 1. Histologic evidence of acute tissue injury, defined by the presence of at least one of the following: a. Glomerulitis (g > 0) or peritubular capillaritis (ptc > 0) b. Intimal or transmural arteritis (v > 0) c. Acute thrombotic microangiopathy of no other obvious cause d. Acute tubular injury of no other obvious cause 2. Current/recent histologic evidence of antibody interaction with vascular endothelium, defined by the presence of at least one of the following: a. Linear C4d staining in peritubular capillaries (at least 10% by immunofluorescence [IF] on frozen sections, or any positivity by immunohistochemistry on paraffin sections) b. At least moderate microvascular inflammation (g + ptc ≥ 2) c. Increased expression of tissue gene transcripts indicative of endothelial injury 3. Presence of donor-specific antibodies (DSA; HLA or non-HLA) in the serum
DSA interact with mismatched HLA or non-HLA molecules primarily on the surface of allograft endothelial cells, leading to cellular injury chiefly through activation of the classical complement pathway. However, antibody-mediated cellular injury through mechanisms other than the classical complement pathway may be involved, as suggested by C4d-negative antibody-mediated rejection. Endothelial injury is followed by microvascular inflammation, endothelialitis, or, if more severe, thrombotic microangiopathy. Sustained endothelial injury will lead to chronic active antibody-mediated rejection.
Glomerulitis can also be seen in immune complex glomerulonephritis or renal vein thrombosis, but the presence of immune complex deposits by IF and electron microscopy in the former and appropriate clinical history in the latter can rule out those conditions. Peritubular capillaritis can also be seen in acute T-cell–mediated rejection, acute tubular injury, and infections.
Endothelialitis (also called intimal arteritis) is a typical feature of T-cell–mediated rejection involving arteries and only recently has been recognized as a feature of antibody-mediated rejection.
Thrombotic microangiopathy can also be seen in other conditions affecting the transplant, such as drug toxicity (eg, calcineurin inhibitor toxicity), recurrent and de novo thrombotic microangiopathic diseases, viral infections (eg, parvovirus B19), or disseminated intravascular coagulation (more often diffuse).
Acute tubular injury is a common and nonspecific lesion in transplant biopsies. It is often difficult to confidently attribute this lesion to antibody-mediated rejection.
Linear C4d staining of peritubular capillaries in the absence of evidence of acute tissue injury can be seen in accommodation, which is common in blood group ABO-mismatched transplants.
Granular C4d staining of peritubular capillaries can be seen in lupus nephritis.