Microscopy Images
Chronic interstitial nephritis is a nonspecific diagnosis of a pattern of kidney injury, which may occur due to any of many conditions that initially cause an acute interstitial nephritis. The diagnosis is made when specific underlying causes cannot be identified.
Patients may present at any age, usually with low-grade proteinuria and slowly progressive decline in glomerular filtration rate, and may reach end-stage kidney disease. Fanconi syndrome may be present, with glycosuria and aminoaciduria.
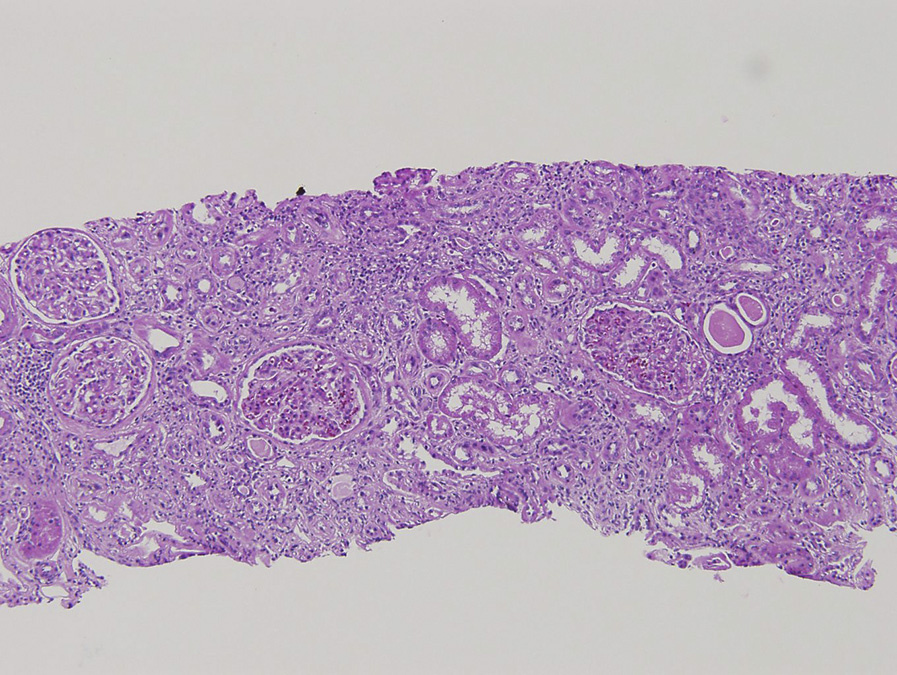
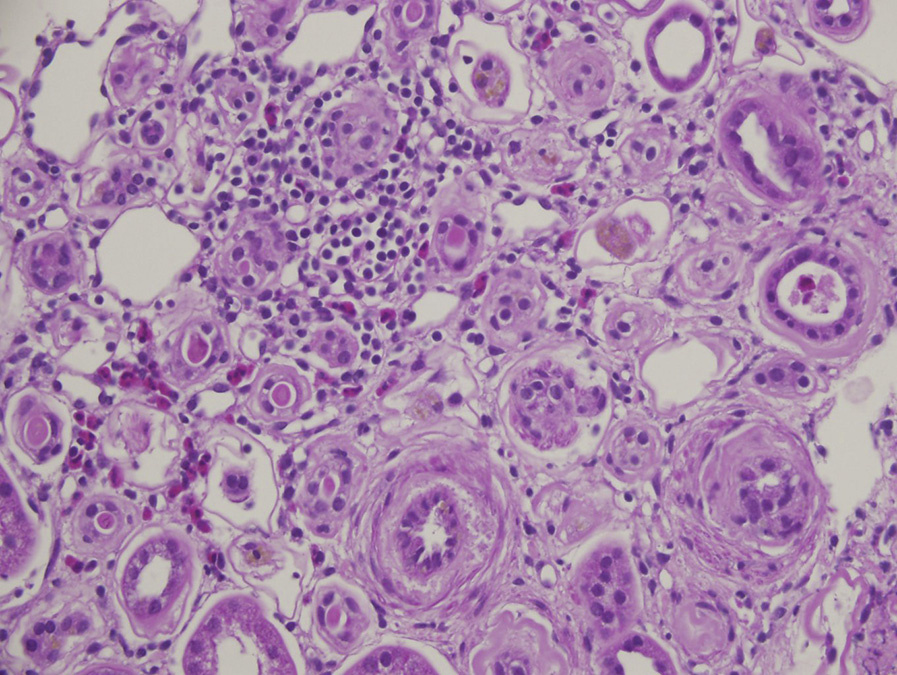
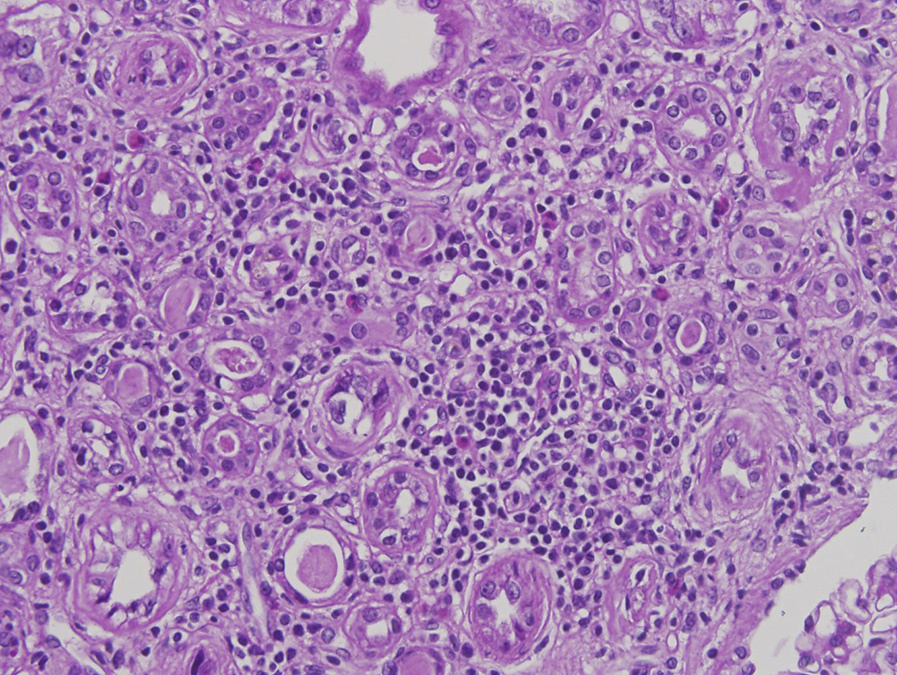
Light microscopy: Biopsies show chronic interstitial nephritis with a lymphoplasmacytic infiltrate out of proportion to the degree of interstitial fibrosis and tubular atrophy. The infiltrate consists of CD4/CD8 T-cells, B-cells, and plasma cells, with scattered tubulitis. Glomeruli are initially unremarkable, but may show periglomerular fibrosis and ischemic wrinkling of glomerular basement membranes and even sclerosis in advanced cases. Vascular sclerosis and hyalinosis may be present.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: No specific changes.
Chronic interstitial nephritis can be caused by many different etiologies, which sometimes can be distinguished based on disease-specific findings.
Thus, chronic interstitial nephritis is a nonspecific term used to describe the lesions described in the previous section when etiology is not apparent.
Common causes are drug-induced hypersensitivity reaction, but specific diagnostic features characteristic of this process are typically lacking at this advanced chronic stage.
Chronic interstitial nephritis may be present in tubulointerstitial nephritis with uveitis syndrome, which is distinguished by the clinical setting. In sarcoidosis, granulomas are common.
Lymphoplasmacytic infiltrates are present in Sjögren syndrome, which is also distinguished by the clinical setting.
Hypersensitivity reactions can be diagnosed when there is residual tubulitis with increased eosinophils and areas of edema, in addition to the chronic changes.
Of note, increased eosinophils appear to be part of nonspecific scarring in the tubulointerstitium in diabetic nephropathy. In IgG4-related disease, there are ≥10 IgG4 positive plasma cells per high-power field, associated with a whorling storiform pattern of fibrosis. Light chain cast nephropathy causes chronic interstitial nephritis and is diagnosed by characteristic fractured intratubular casts appearance and a syncytial cell reaction to the casts, often with monoclonal staining for either κ or λ light chain subclass. Obstruction with extrusion of uromodulin (Tamm-Horsfall protein) into the interstitium can cause local chronic interstitial nephritis. Tubular deposits, crystals, and viral or other infections each are distinguished by disease-specific findings (see specific entities for details).