Microscopy Images
Cytomegalovirus is a double-stranded DNA virus that is a member of the herpesvirus family. Most people are CMV positive, with latency established in hematopoietic cells after primary infection. Immunosuppressed patients and kidney transplant recipients are particularly vulnerable. Seropositive recipients of a seropositive transplant are treated with prophylaxis, and seronegative individuals may have primary infection. Reactivation of the latent virus in the kidney transplant patient can result in a severe systemic illness, with fever, multiple organ dysfunction with associated leukopenia, and CMV in the blood.
Commonly involved organs include the gastrointestinal tract, liver, lung, kidneys, and central nervous system. Patients present with acute kidney injury in the setting of findings of systemic infection. Patients may respond to antiviral therapy, with worse outcome in infected patients without such therapy. CMV infection is also associated with increased risk for acute rejection.
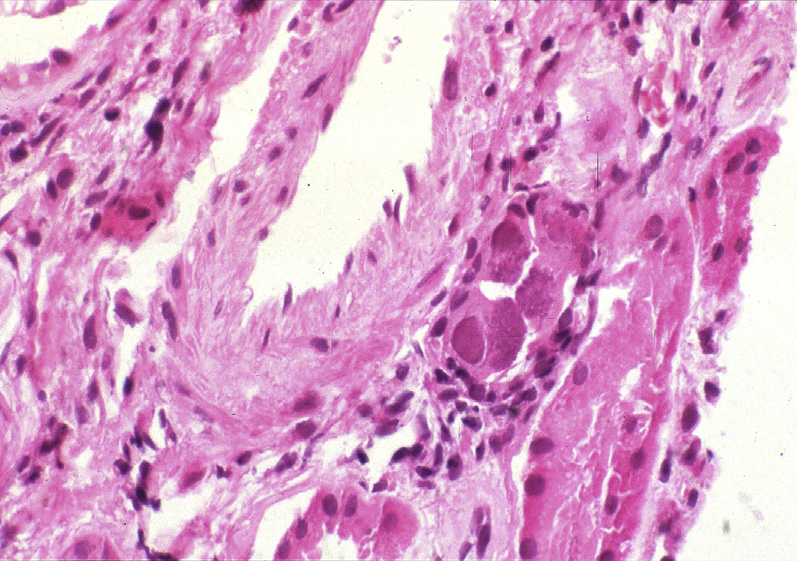
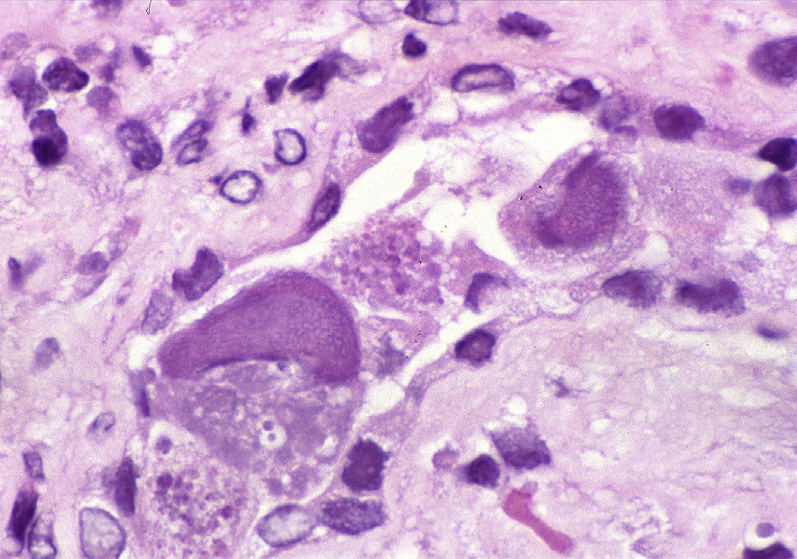
Light microscopy: There is patchy interstitial pleomorphic infiltrate with lymphocytes, plasma cells, and macrophages. Tubulitis is present, with characteristic intranuclear glassy-appearing basophilic inclusions with surrounding halo (owl’s eye-type inclusion) and marked increase in the size of the cell (cytomegaly), particularly in tubular epithelial cells and in endothelial cells. Glomerular epithelial cells also can rarely be infected. Specific diagnosis is confirmed by immunohistochemical staining for CMV.
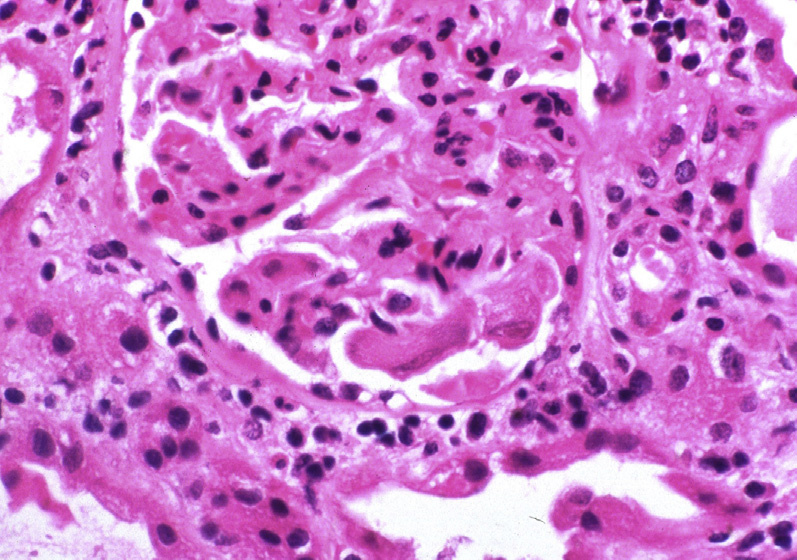
Glomerular involvement is commonly without inflammatory influx, but rarely is associated with endocapillary hypercellularity. CMV arteriopathy can present as thrombotic microangiopathy.
Immunofluorescence microscopy: There are no specific staining patterns.
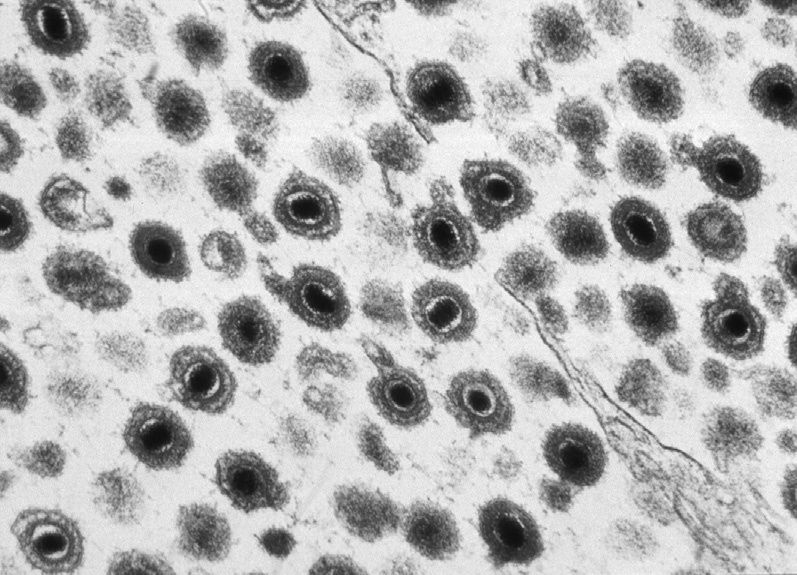
Electron microscopy: Viral particles, 150-200 nm in diameter, may be seen both in the nucleus and in the cytoplasm of infected cells, and have a dense central core and thick capsule. In the cytoplasm, a characteristic additional membrane is present due to the nuclear membrane as the particles transit from the nucleus to the cytoplasm.
Acute cellular rejection does not have viral cytopathic changes or positive CMV staining. Other viruses are diagnosed by specific immunohistochemistry or in situ hybridization. When glomeruli are infected, endothelial cell injury could overlap with that seen in chronic transplant glomerulopathy, but the latter has no viral inclusions or immunohistochemistry positivity for CMV.