Microscopy Images
Polyomavirus infection occurs in the transplanted allograft kidney and in the native kidney of immunosuppressed patients, and is usually related to BK virus (80%), JC virus (10%-20%), and less frequently simian virus 40 (SV40). Polyomaviruses are DNA and nonenveloped, with tropism for the urothelium.
Transplanted kidneys have about 5% infection prevalence. Polyomavirus nephropathy usually presents as an asymptomatic acute or slowly rising creatinine.
Polyomavirus infection can also present as nonhemorrhagic or hemorrhagic cystitis, and rarely as ureteral obstruction.
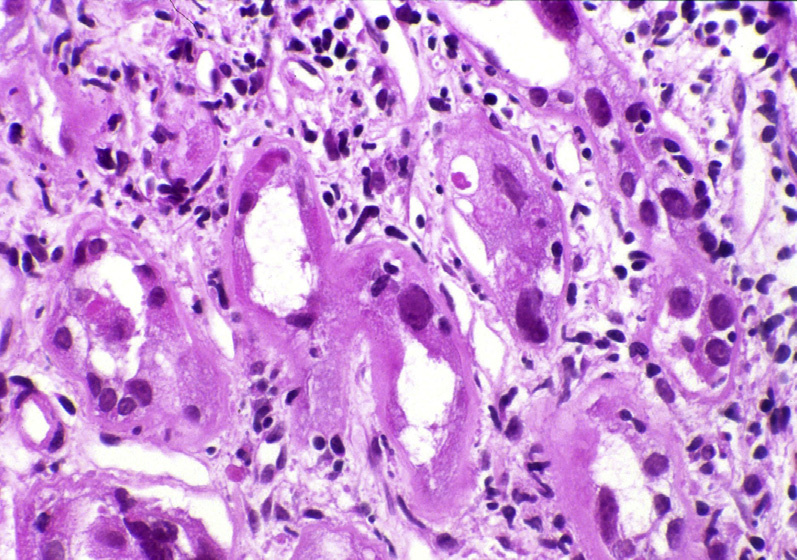
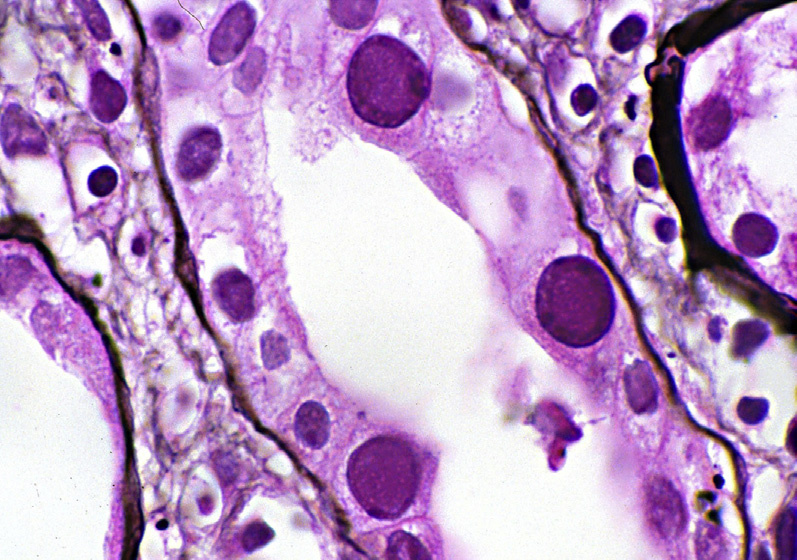
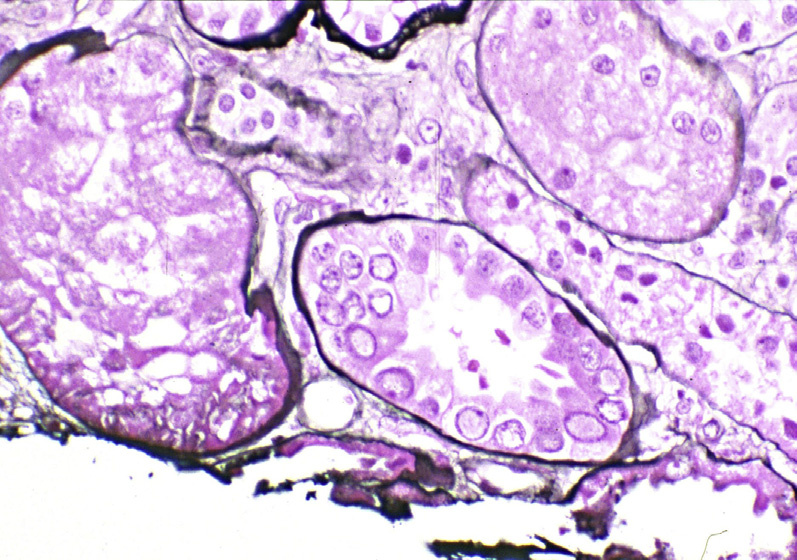
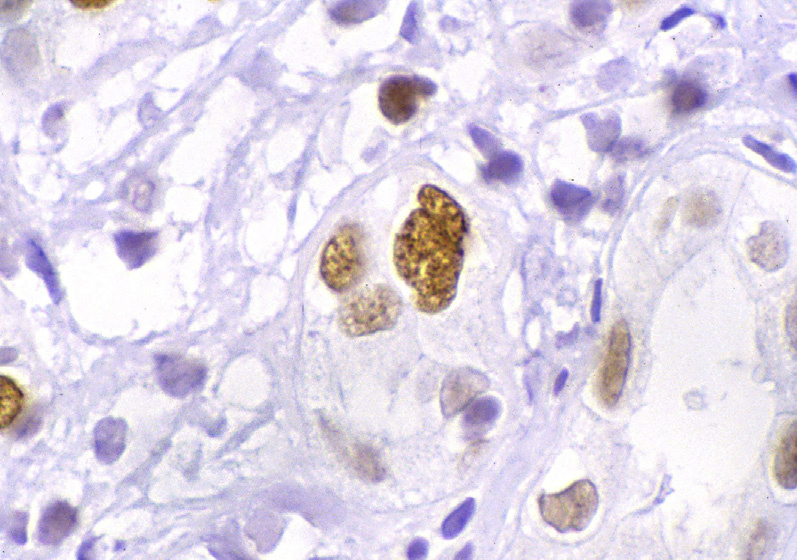
Light microscopy: There is a patchy pleomorphic interstitial infiltrate with lymphocytes, plasma cells, and occasional neutrophils with associated interstitial edema, tubulitis, and tubular injury. Infected tubular epithelial cells have enlarged nuclei with amorphous inclusions. These nuclear inclusions have a ground-glass appearance with irregular central clearing, or a coarse, vesicular appearance. Distal tubules are involved more often than proximal tubules. There may be only medullary involvement in early stages, and parietal epithelial cells may be involved in later stages of the infection. Infected epithelial cell nuclei stain with antibody to the large T antigen of the SV40 virus, which serves as a surrogate marker of human polyomavirus infection.
Positive staining may be seen in the absence of nuclear enlargement or inclusions.
Immunofluorescence microscopy: Granular tubular basement membrane (TBM) staining for IgG, C3, and C4d may be present in up to 10%-25% of cases.
Electron microscopy: Polyomavirus particles, 30-45 nm, are present in nuclei of infected cells, sometimes with a lattice-like arrangement. Rare cytoplasmic viral particles may be present. In cases with TBM granular staining by immunofluorescence, immune complex–type deposits are present along TBM.
Polyomavirus nephropathy mostly represents a reactivation of latent virus in infected kidney epithelial cells, particularly tubular epithelial and urothelial cells.
Viral infections caused by herpes simplex virus (HSV), adenovirus, and cytomegalovirus (CMV) can cause viral cytopathic changes that can overlap with polyomavirus-related cytopathic changes.
HSV is typically associated with multinucleated giant cells with nuclear inclusions and may cause hemorrhagic interstitial nephritis. Adenovirus has basophilic nuclear inclusions and is associated with interstitial hemorrhage, necrosis, and rarely granulomas. CMV typically infects endothelial cells.
Specific immunostaining will distinguish between these infections from polyomavirus-related infection.
Acute cellular rejection (ACR)-related interstitial infiltrate is composed predominantly of T cells without viral cytopathic changes within tubular epithelial cells. Plasma cell–rich ACR is distinguished from polyomavirus nephropathy by lack of SV40 staining. Concomitant ACR and polyomavirus nephropathy can occur.
Presence of vascular rejection with endothelialitis is diagnostic for concomitant T cell–mediated rejection, even if polyomavirus nephropathy is confirmed by SV40 staining. Acute interstitial nephritis due to drug hypersensitivity reaction may have more frequent interstitial eosinophils, with no viral cytopathic changes and absence of staining for SV40.