Microscopy Images
Fibronectin glomerulopathy usually presents in the second to fourth decade of life with nephrotic-range proteinuria, microscopic hematuria, and hypertension, with fewer than half of patients showing mild decreases in kidney function. Decline of kidney function over time is variable. Serum fibronectin levels are usually normal and systemic manifestations have not been reported. Recurrence in the transplant may occur.
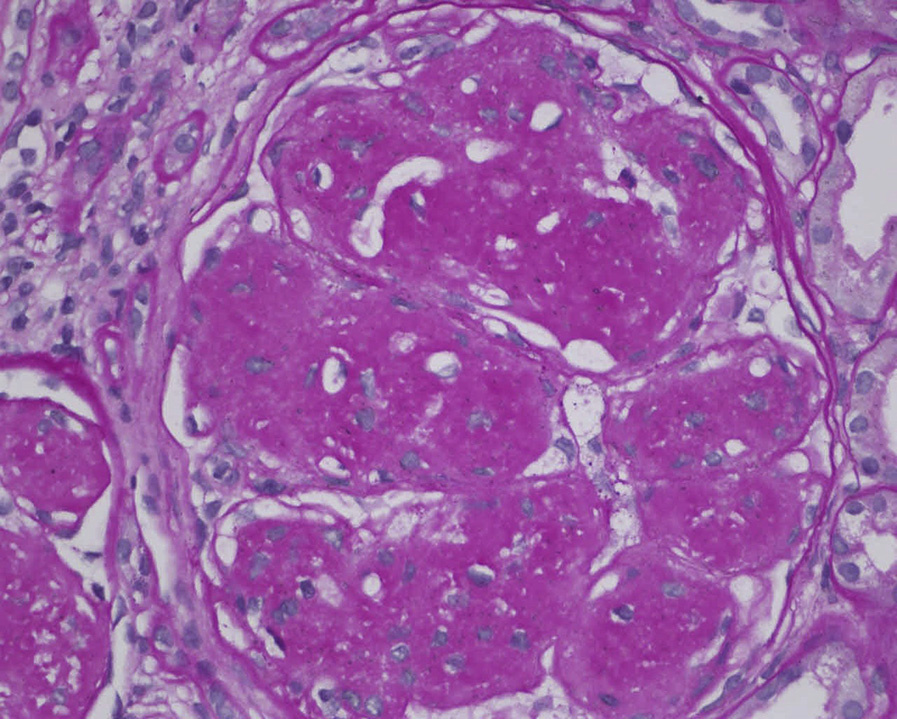
Light microscopy: There is lobular accentuation with mesangial expansion with minimal hypercellularity and variable expansion of glomerular basement membranes by strongly periodic acid–Schiff–positive and silver-negative material. Congo red stain is negative.
There are nonspecific tubulointerstitial and vascular changes with increased fibrosis with progression of disease.
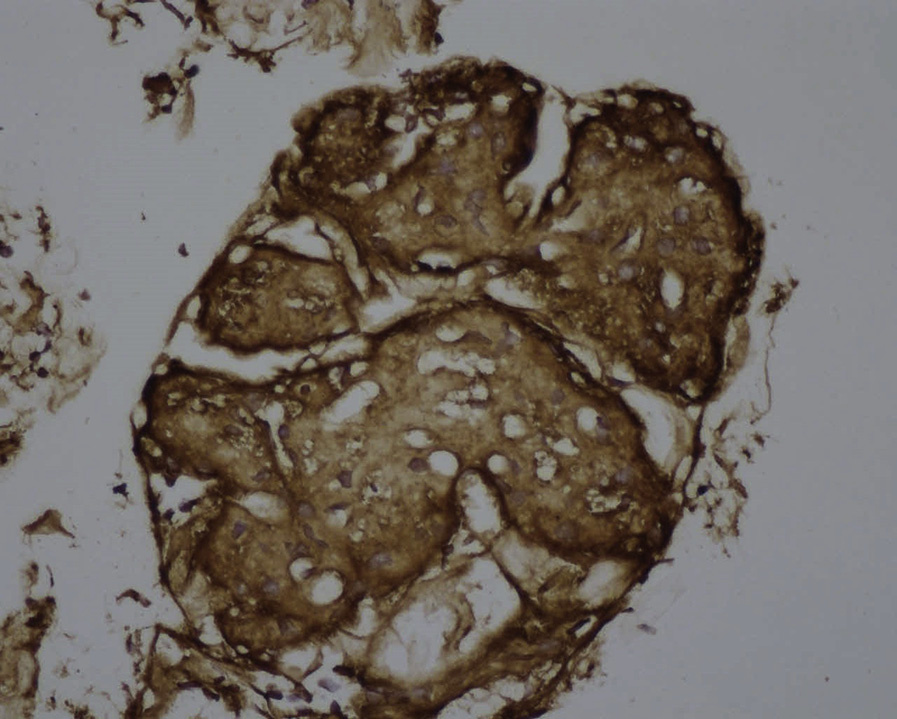
Immunofluorescence/immunohistochemistry microscopy: Usually negative, but may show nonspecific staining for immunoglobulins and C3. Fibronectin immunochemistry stain is strongly positive in deposits.
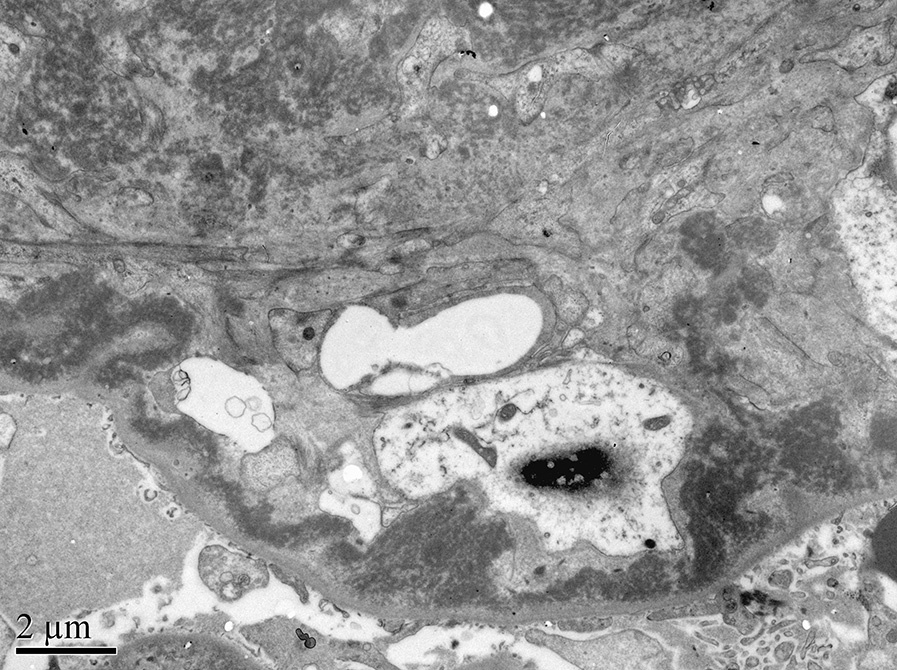
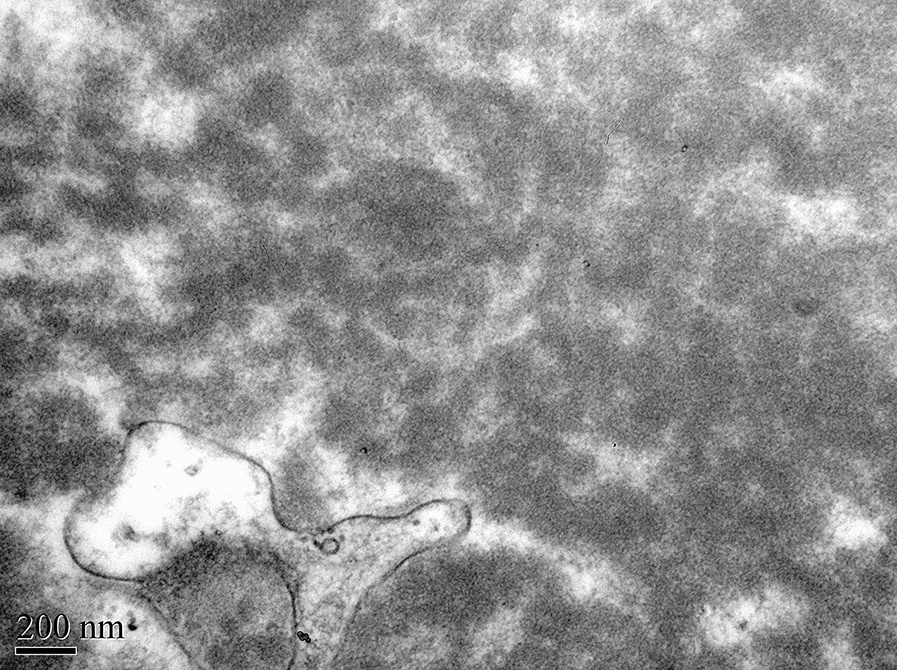
Electron microscopy: There are massive mesangial and subendothelial deposits, which may show focal fibrillary substructure with a fibril diameter of 12-16 nm.
Rarely, deposits may involve the tubular basement membranes and Bowman capsule.
Fibronectin glomerulopathy is an autosomal dominant disease with age-related penetrance. About 40% of patients have a mutation involving the fibronectin gene (FN1), which maps to chromosome 2q34.
Fibronectin is a high-molecular-weight glycoprotein component of the extracellular matrix that can bind to heparin and to integrins, that also circulates as a dimer.
It is normally produced by the liver and renal mesangial cells. The pathogenic mechanism of fibronectin accumulation is not completely understood, but may involve the production of a fibronectin variant that cannot be cleared, or the formation of a variant fibronectin formed by attachment of a circulating factor.
The deposits consist predominantly of the soluble plasma-derived form of fibronectin, rather than the insoluble cellular form. In vitro, this variant fibronectin shows deficient binding to heparin on the surface of podocytes and endothelial cells, resulting in impaired capability to induce endothelial cell spreading and podocyte cytoskeleton reorganization. Another proposed mechanism is a defect in the catabolism of fibronectin. Fibulin 1 and 5, which can bind and/or regulate fibronectin, are also at increased levels and are present in the deposits.
Lobular glomerular appearance also occurs in immune complex–mediated glomerulonephritis with membranoproliferative pattern of injury, with disease-specific immunofluorescence staining with usual type immune complex deposits by electron microscopy.
Amyloidosis can have a lobular pattern glomerular injury. Amyloid deposits are weakly periodic acid–Schiff–positive and are congophilic with apple-green birefringence under polarized light by Congo red stain with nonbranching randomly arranged fibrils of 8-12-nm diameter. Fibrillary glomerulopathy deposits have fibrillary substructure with nonbranching fibrils of 10-30 nm diameter with mesangial, sometimes subendothelial and occasional subepithelial deposition with immunoglobulin, most often polyclonal, and complement deposition by immunofluorescence.
Immunotactoid glomerulopathy deposits are microtubules of >30-nm diameter in parallel arrays, with immunoglobulin (typically monoclonal) and complement deposition. Monoclonal immunoglobulin deposition diseases show lobular expansion of mesangial matrix by light microscopy with light and/or heavy chain staining restriction along glomerular and tubular basement membranes by immunofluorescence with granular, often confluent, electron-dense deposits that typically have either an amorphous or powdery appearance by electron microscopy. Type III collagen glomerulopathy shows enlarged glomeruli with lobular appearance with pale periodic acid–Schiff staining without immunoglobulin or complement by immunofluorescence, with characteristic collagen type III deposits composed of whorling and cross-striated fibrils with about 60-nm periodicity.
Diabetic nephropathy has characteristic Kimmelstiel-Wilson nodules with thickened glomerular basement membranes by electron microscopy without immune complex deposits.