Microscopy Images
The Columbia classification of focal segmental glomerulosclerosis (FSGS) describes 5 variants.
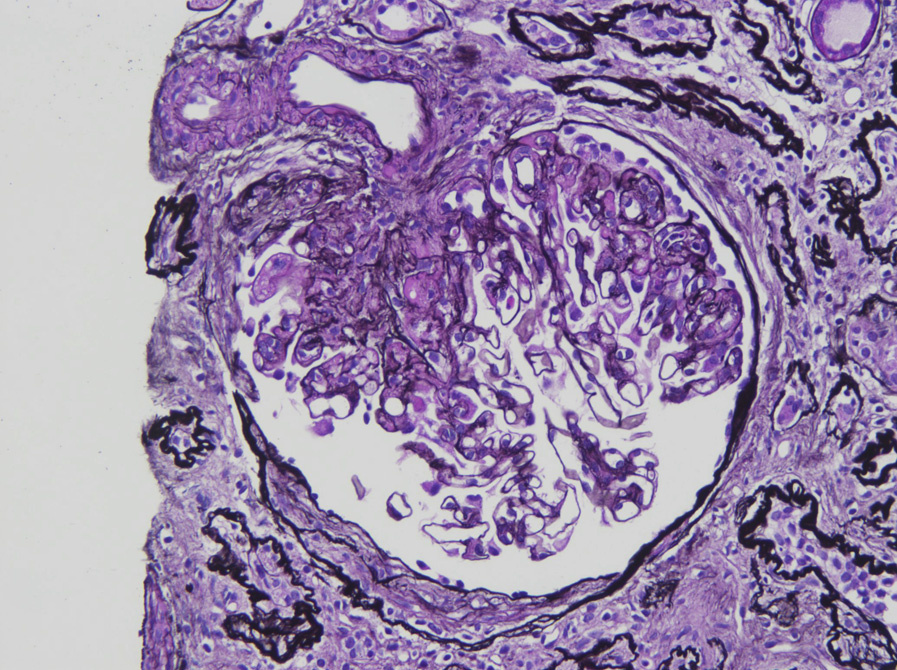
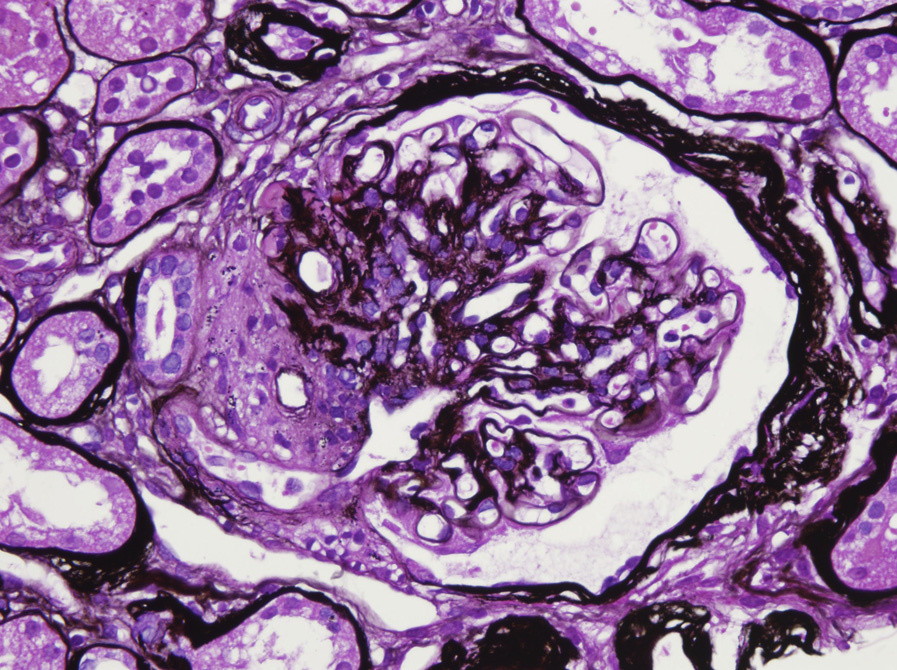
The hilar variant is more common in adults, and typically presents with subnephrotic-range proteinuria. The hilar variant can be diagnosed after excluding the collapsing, tip, and cellular variants, when there is segmental sclerosis at the vascular pole (hilum) in most of the involved glomeruli.
There is an absence of immune complexes. Prognosis is intermediate between collapsing (worst) and tip (best) variants of FSGS, but usually with no response to immunosuppression.
Light microscopy: Hilar sclerosis, often with hyalinosis. Glomerulomegaly may be present.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: Foot process effacement, which may be more limited than in other primary FSGS variants, without deposits.
Hilar FSGS is believed to develop as an adaptive response after the loss of nephrons. It may also be associated with hypertension. The injury could represent primary FSGS, or more often, secondary etiologies, including obesity-related glomerulopathy or anabolic steroid use.
The hilar variant of FSGS may occur in a variety of settings (discussed above). Small glomeruli with corrugation of glomerular basement membranes, increased lamina rara interna revealed by electron microscopy, and severe vascular sclerosis, often with extensive solidified type of global glomerulosclerosis, are typical of the hilar FSGS associated with hypertension. Hilar FSGS related to loss of nephrons or obesity often has glomerulomegaly.