Microscopy Images
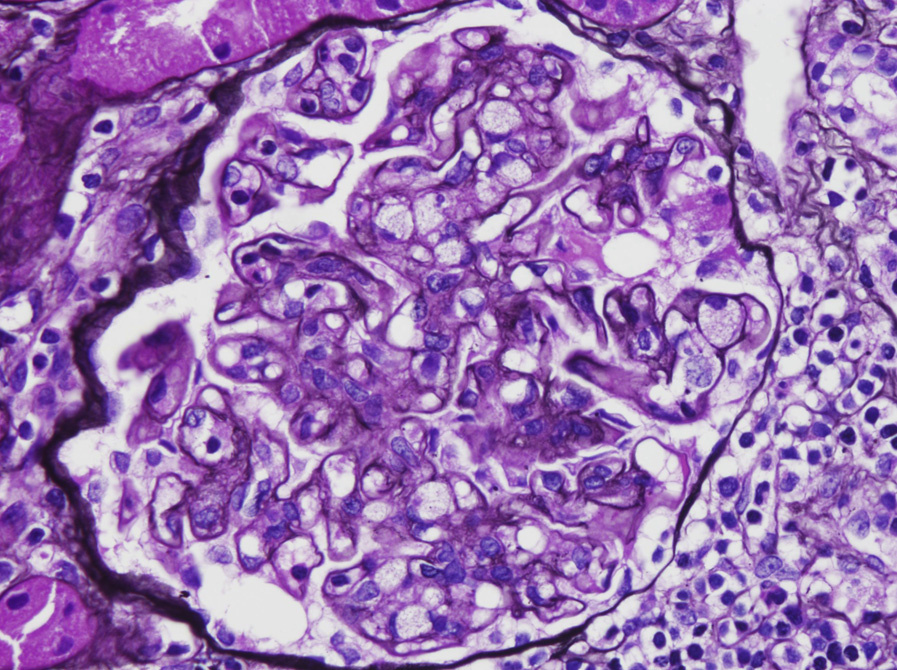
The Columbia classification of focal segmental glomerulosclerosis (FSGS) describes 5 variants, of which the cellular variant is the rarest. This variant is more common in children than in adults, and typically presents with nephrotic-range proteinuria. The cellular variant can be diagnosed after excluding collapsing and tip variants, when there is endocapillary hypercellularity involving at least 25% of the tuft of at least one glomerulus, without immune complexes, and typically with extensive foot process effacement.
Prognosis is intermediate between the worst outcomes seen with the collapsing variant versus the best prognosis observed with the tip variant.
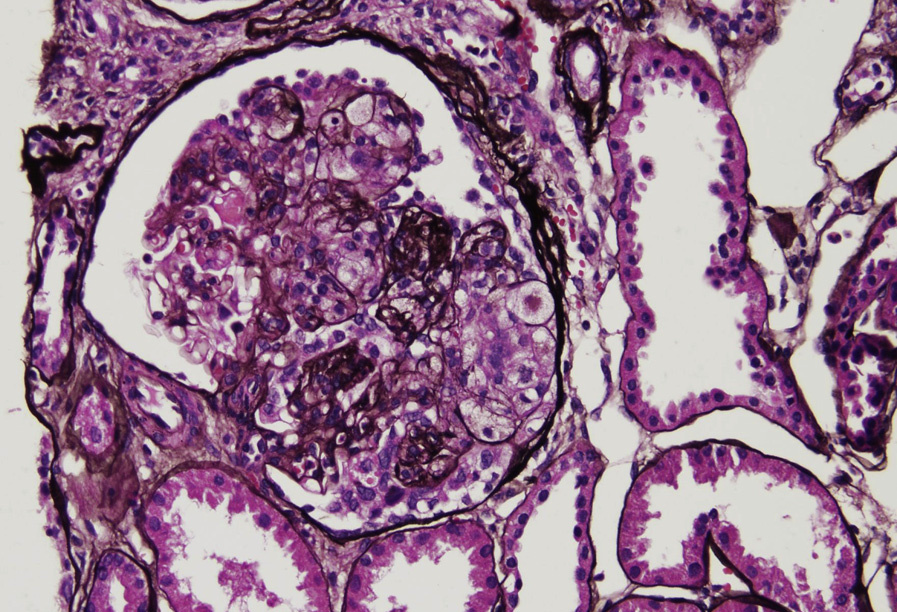
Light microscopy: Segmental or global endocapillary hypercellularity, most often focal with usual sclerosis in other glomeruli, foam cells, and overlying hyperplastic visceral epithelial cells.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: Extensive foot process effacement without deposits.
This cellular variant lesion might be an early abnormality revealed by light microscopy for recurrent FSGS in a kidney transplant. Additional sections may reveal that some of these cellular lesions involve the tubular pole, and thus are better classified as tip lesion variant FSGS.
The presence of endocapillary hypercellularity revealed by light microscopy suggests possible immune complexes, which can readily be ruled out by lack of deposits shown by immunofluorescence and electron microscopy. Multiple serial sections are required to assess for possible tip lesions.