Microscopy Images

Idiopathic nodular sclerosis (INS) has a predilection for older white men. Patients usually present with reduced GFR and nephrotic-range proteinuria.
Often patients have a clinical history of hypertension, tobacco use, hypercholesterolemia, and vascular disease. A clinical history of diabetes must be excluded.
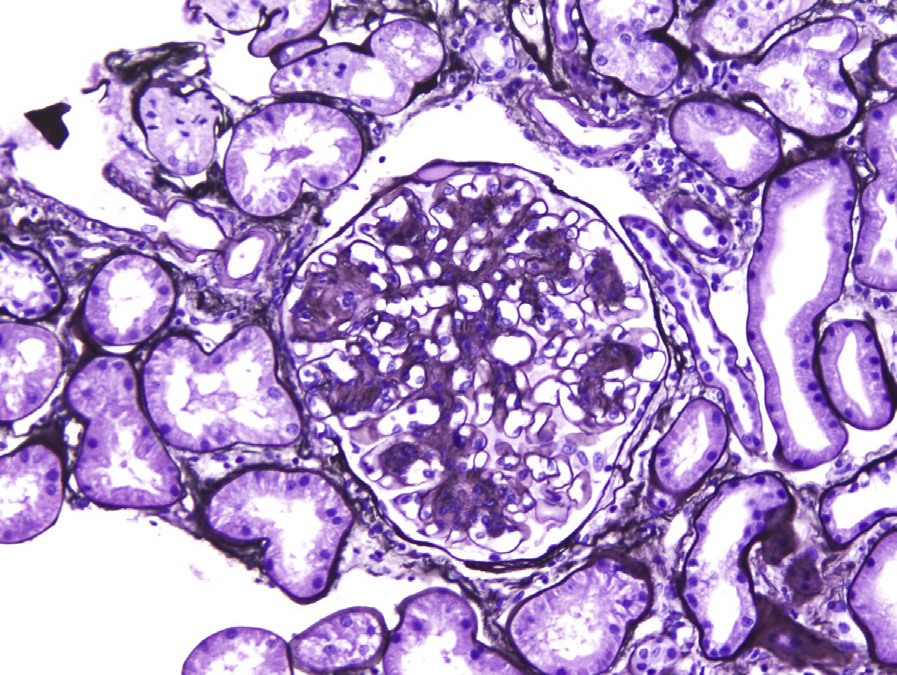
Light microscopy: Glomerulomegaly with diffuse nodular mesangial expansion that may be associated with microaneurysms, indistinguishable from that seen in diabetic nephropathy. There is arteriolar hyalinosis and often moderate arteriolosclerosis.
Capsular drops may be present. There is proportional tubulointerstitial fibrosis.
Immunofluorescence microscopy: IgG and albumin linear accentuation of glomerular basement membranes may be present. No immune deposits.
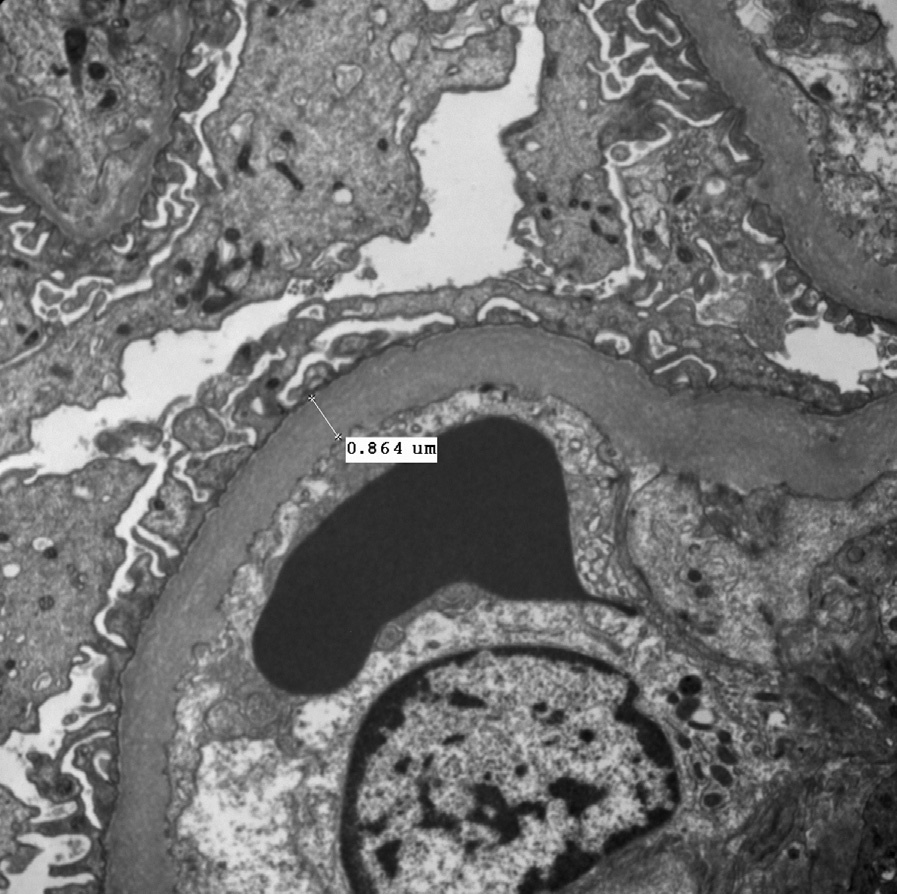
Electron microscopy: Mesangium is expanded by increased matrix and glomerular basement membranes are typically moderately thickened with variable foot process effacement. No immune deposits.
INS has been associated with hypertension and tobacco use. Smoking is postulated to induce nodular glomerulosclerosis through the formation of advanced glycosylation end products with induction of oxidative stress and angiogenesis with altered intrarenal hemodynamics.
Hypertension-related injury may represent a pre-existing insult.
INS has morphologic findings identical to diabetic nephropathy, and can only be distinguished by excluding a clinical history of diabetes. Monoclonal immunoglobulin deposition disease can also have nodular sclerosis, with monoclonal immune linear staining by immunofluorescence and granular amorphous deposits by electron microscopy along glomerular and tubular basement membranes, features not seen in INS. Amyloidosis nodular mesangial expansion is due to amorphous, eosinophilic, acellular material that shows characteristic apple-green birefringence under polarized light on Congo Red stain, with fibrillary deposits composed of nonbranching, randomly arranged fibrils by electron microscopy. Membranoproliferative glomerulonephritis can have nodular lesions, but has disease-specific immunofluorescence and electron microscopy findings.