Microscopy Images
Karyomegalic nephropathy is a rare autosomal recessive disease due to mutation in the FAN1 gene, resulting in low-grade proteinuria and slowly progressive GFR loss starting in the third decade of life, culminating in end-stage kidney disease.
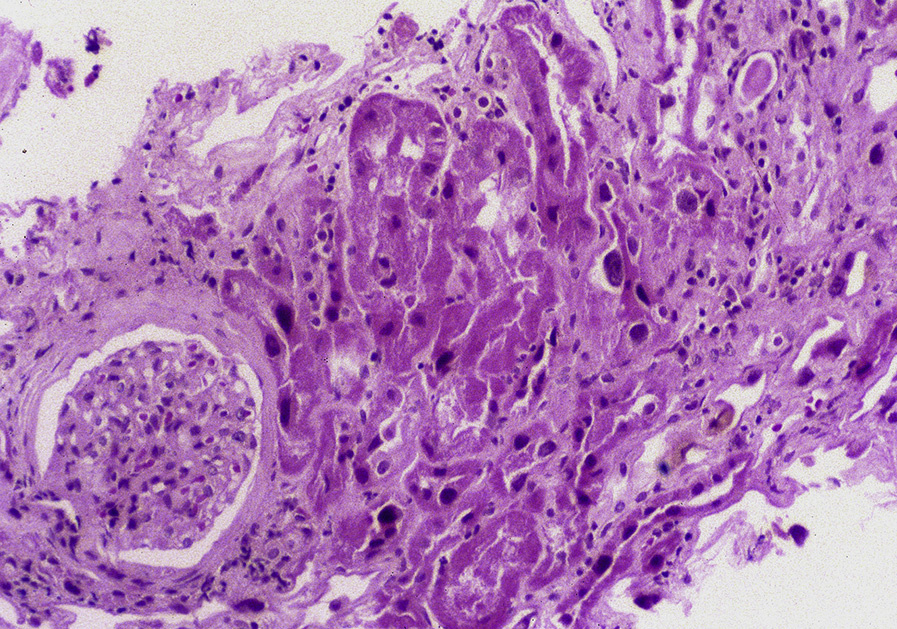
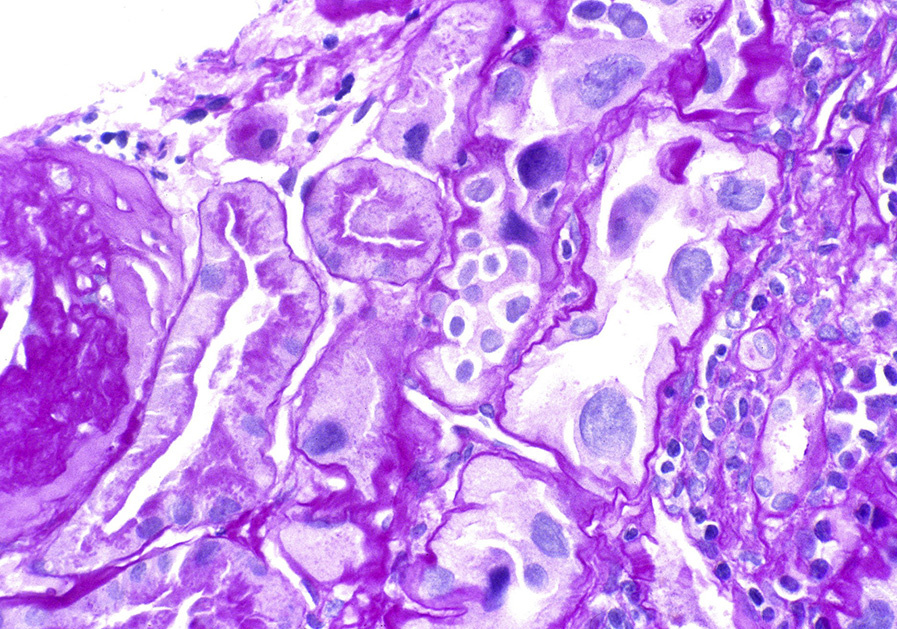
Light microscopy: There are bizarre, enlarged proximal tubular nuclei with varying tubular atrophy and interstitial fibrosis. There may be microcystic tubular dilation and variable interstitial mononuclear cell infiltration. Glomeruli are typically unremarkable.
Immunofluorescence microscopy: Noncontributory.
Electron microscopy: Proximal tubular basement membranes are thickened without deposits.
Karyomegalic nephropathy is due to mutation in FAN1, which plays a key role in DNA repair. Additional environmental insults, such as ochratoxin, with inadequate DNA repair are postulated to cause the morphologic lesions. Mutations in this gene may also give rise to nephronophthisis in some patients, without the characteristic enlarged tubular nuclei of karyomegalic nephropathy. Although karyomegalic change has been observed in other organs, such as brain, liver, lung, and the gastrointestinal tract, no clinical manifestations have been described in organs other than the kidney.
Enlarged tubular nuclei are present in lead poisoning, but with nuclear inclusions. Viral infections may cause cytomegaly, but the cells are not irregular and bizarre as in karyomegalic nephropathy.
Also, viral inclusions are present, with positive immunostaining/in situ hybridization for the virus (eg, polyoma virus nephropathy, cytomegalovirus nephropathy).