Microscopy Images
Minimal change disease (MCD) is characterized by nephrotic syndrome. It is the most common cause of nephrotic syndrome in children aged 1 to 7 years and remains a cause of nephrotic syndrome in adults.
Kidney function is usually preserved, except for occasional cases with acute kidney injury.
MCD is typically responsive to steroids with excellent long-term prognosis.
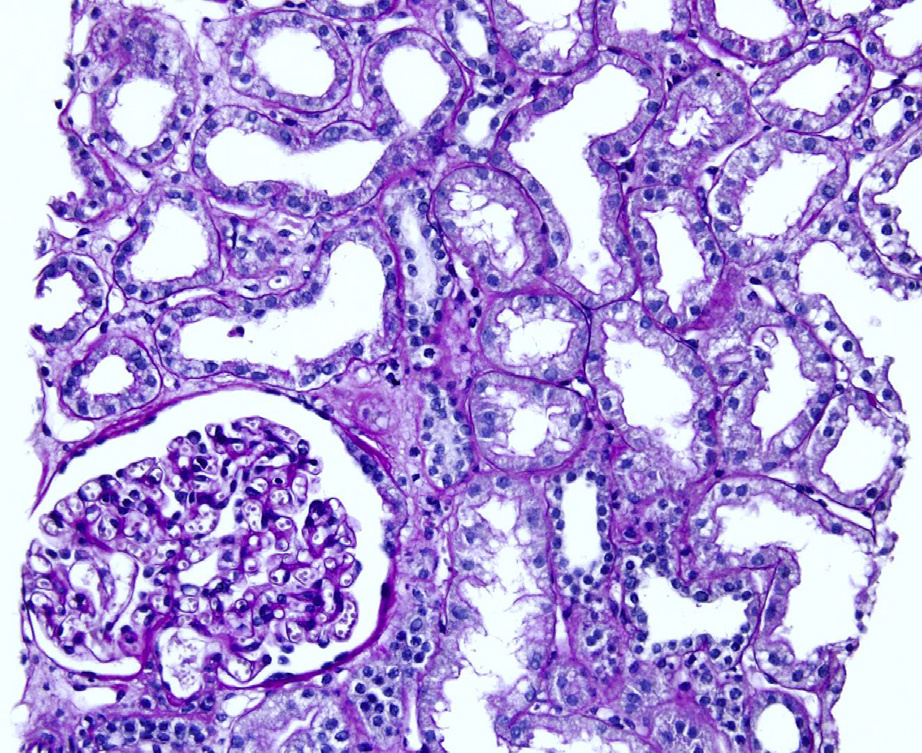
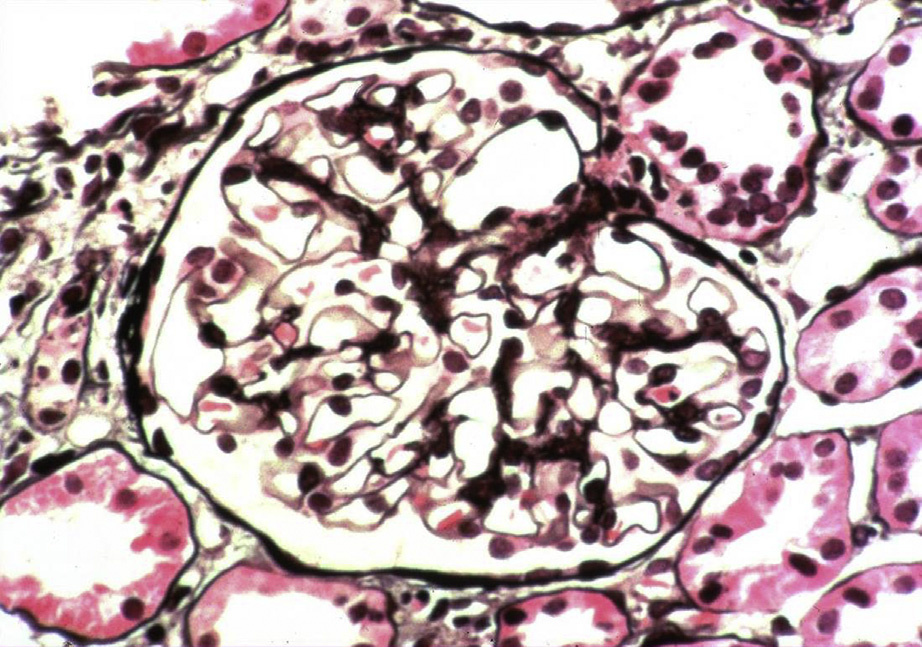
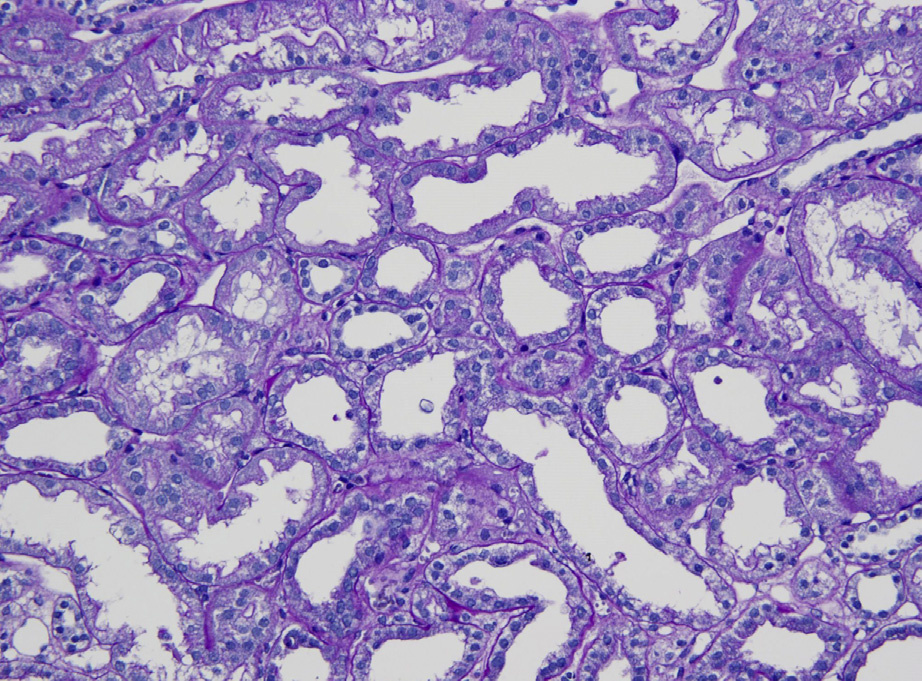
Light microscopy: Unremarkable glomeruli. Of note, global glomerulosclerosis is a nonspecific finding that can be seen.
Immunofluorescence microscopy: No deposits (may have nonspecific immunoglobulin M [IgM]).
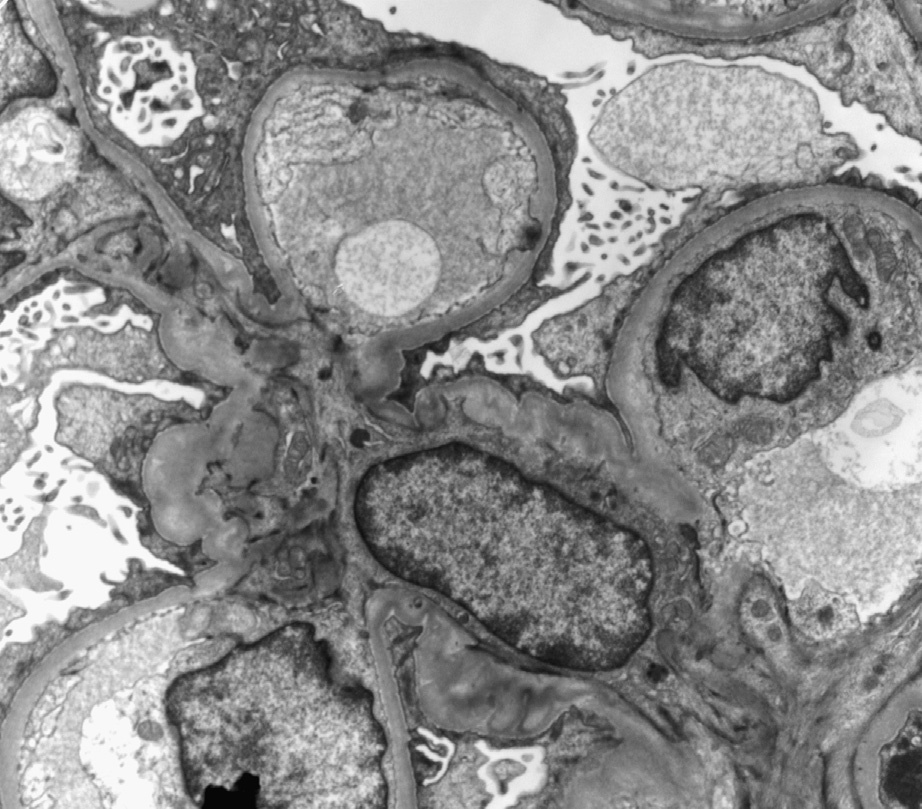
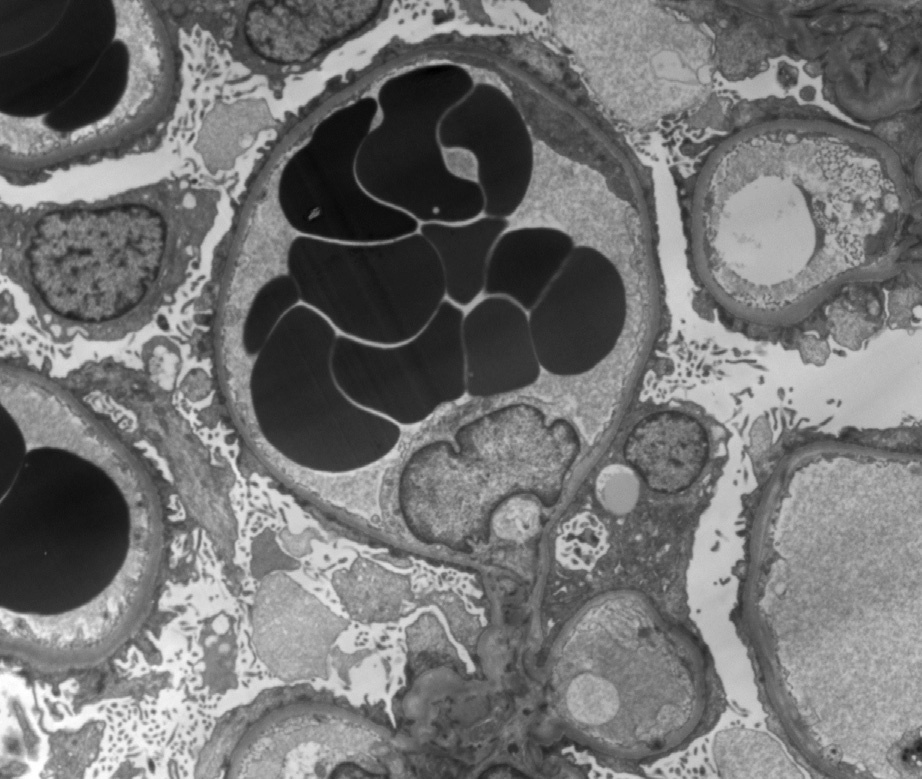
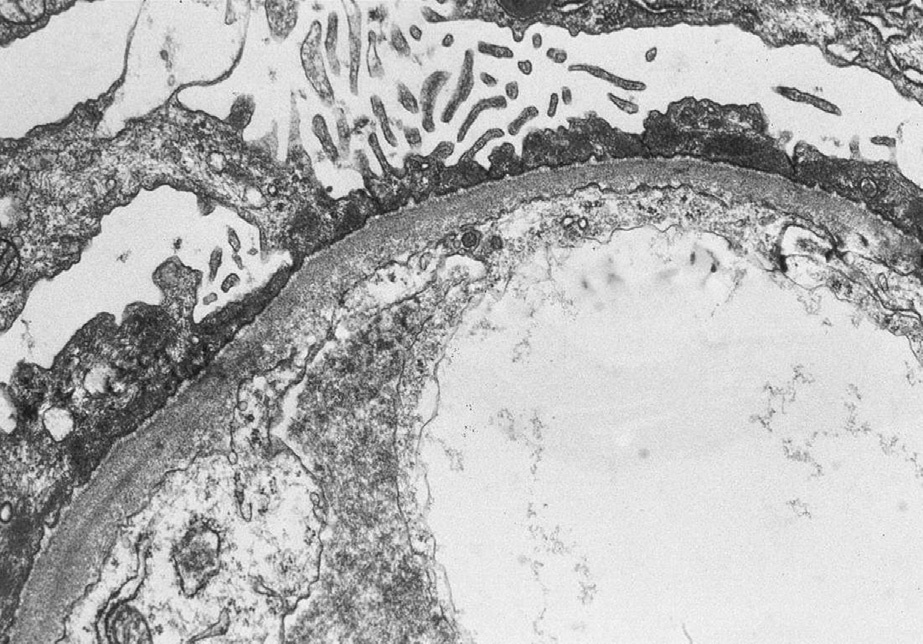
Electron microscopy: Extensive foot process effacement.
Abnormal cytokines from T cells and/or abnormal T-cell regulation by B cells are implicated. These may cause increased CD80 on podocytes in MCD.
MCD may also occur secondary to lymphomas, with hypersensitivity reactions (eg, acute interstitial nephritis from nonsteroidal anti-inflammatory drugs), with HIV (human immunodeficiency virus) infection, or with bee stings. In addition, extensive foot process effacement with nephrotic syndrome has been observed in patients with mild mesangial lupus nephritis and mild IgA nephropathy and may represent MCD-like injury in those patients.
Unsampled focal segmental glomerulosclerosis (FSGS); an adequate sample (ideally >25 glomeruli, including juxtamedullary area) is needed to reasonably exclude FSGS.
Degree of foot process effacement does not differentiate between unsampled primary FSGS and MCD.
Limited foot process effacement (,50%) suggests the process is probably not MCD or primary FSGS, unless the patient has been treated with partial response.
CD44 expression on visceral epithelial cells may indicate activated parietal epithelial cells transitioning to the tuft and could be a sign of early FSGS-type injury.