Microscopy Images
Tubulointerstitial nephritis with uveitis (TINU) accounts for about 5% of interstitial nephritis cases. This syndrome mainly occurs in adolescents (median age of onset is 15 years) and rarely in adults, with a higher prevalence in females than males. Patients may present with tubular dysfunction (including Fanconi syndrome, decreased kidney function, and proteinuria), kidney failure, and ocular symptoms. Uveitis may precede or follow renal involvement. In some cases, bone marrow and lymph node involvement with granulomas can occur. Steroid therapy facilitates recovery, though spontaneous remission can occur.
Persistent disease can lead to permanently decreased kidney function.
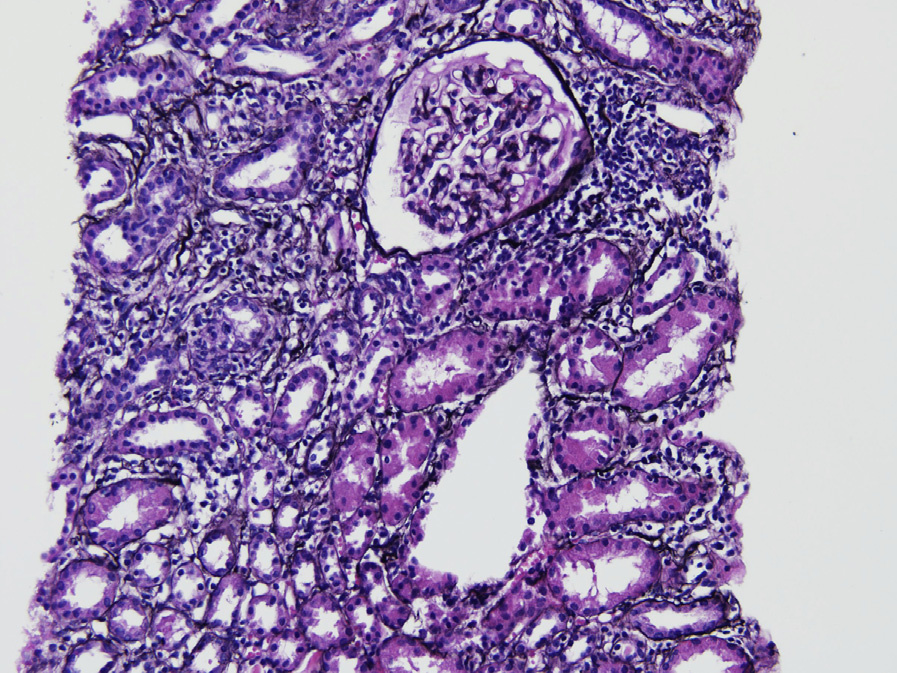
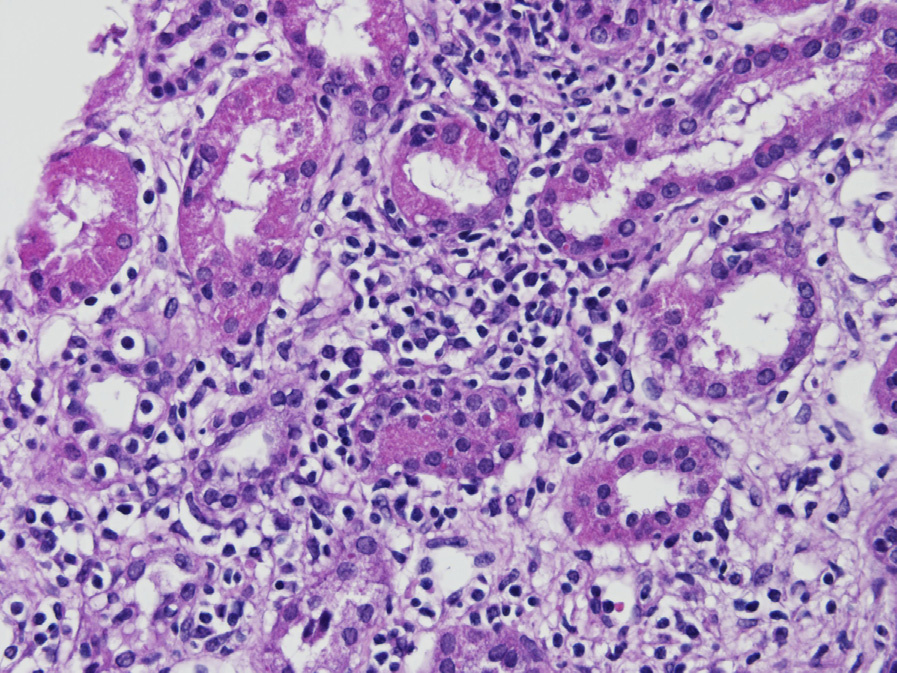
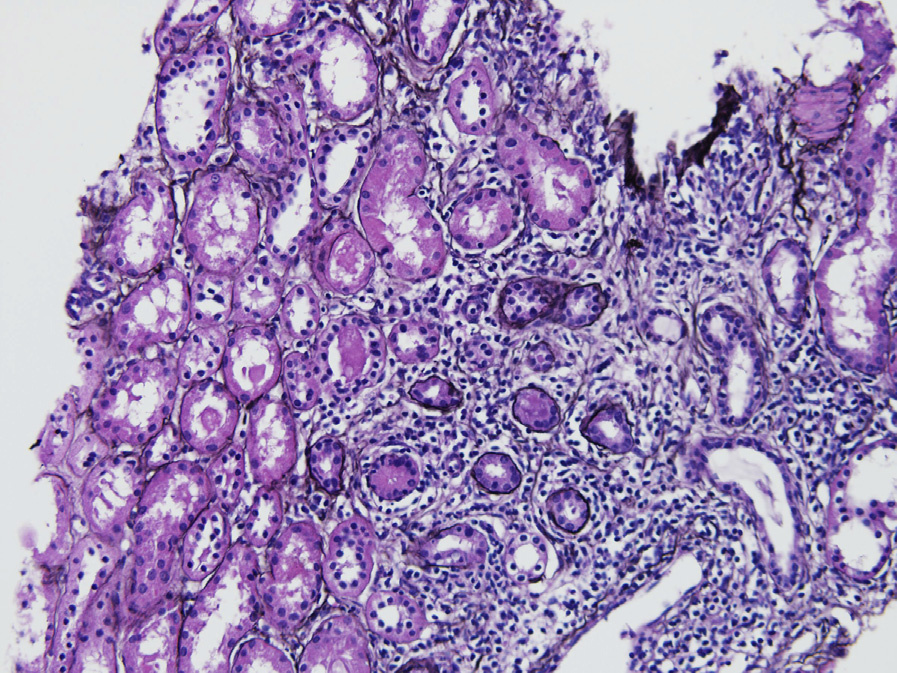
Light microscopy: There is an interstitial infiltrate composed mainly of lymphocytes with fewer plasma cells and macrophages, associated with tubulitis. A prominent eosinophilic infiltrate may be present at initial presentation. Interstitial granulomas, including extensive confluent granulomas, can occur.
As disease progresses, variable amounts of interstitial fibrosis are present with less inflammatory infiltrate. TINU typically has more tubular atrophy than other etiologies of interstitial nephritis.
Immunofluorescence microscopy: Usually without glomerular or tubular staining.
Electron microscopy: Noncontributory.
TINU is most likely related to autoimmune lymphocytic activation and antibodies to renal tubular epithelia, as well as antibodies to uveal cells. The occurrence of cases in identical twins and siblings with identical haplotypes suggests a genetic predisposition.
Environmental exposures may play a role. Infectious etiologies have been suggested to trigger TINU, including Klebsiella, Chlamydia, Mycoplasma, herpes zoster, Epstein-Barr virus, and Toxoplasma.
Drug-induced acute interstitial nephritis is morphologically indistinguishable from TINU. In the former there typically are more numerous interstitial eosinophils and a history of drug exposure, with skin rash and absence of uveitis.
Sarcoidosis morphologically has prominent and confluent granulomas, which is less common in TINU.
Sjögren syndrome clinically presents with xerostomia, xerophthalmia, and antinuclear antibody positivity, while TINU does not.