Microscopy Images
![AL amyloidosis with λ light chain–restricted staining in glomeruli, arteries, and interstitium (immunofluorescence microscopy, staining for [A] κ and [B] λ light chains).](../assets/AL_Amyloidosis_003.jpg)
Amyloidosis is a systemic disease caused by amyloid deposition, which may be due to a monoclonal protein, hereditary disorders, or other conditions (see also Hereditary and Other Non-AL Amyloidoses). The type is diagnosed by immunofluorescence (IF), immunohistochemistry, or mass spectrometry. Patients with AL amyloid are middle-aged or older adults. Kidney involvement by AL amyloid typically manifests by nephrotic syndrome. Patients may also show signs related to the underlying plasma cell dyscrasia, such as anemia, and other organ involvement, which may manifest as neuropathy, heart failure with arrhythmias, hepatosplenomegaly, and more rarely macroglossia.
AL amyloid in the kidney deposits in glomeruli and often in vessels. Interstitial amyloid is clinically evident as a concentrating defect. Some patients (around 15%) have concomitant light chain cast nephropathy caused by the monoclonal protein, with resulting acute kidney injury. Patients who are eligible for treatment of the underlying plasma cell dyscrasia/multiple myeloma have hematologic response in about half of cases, with corresponding stabilization or even improvement of end-organ function related to amyloid. Median survival in such patients is around 4.5 years. In patients who are not eligible for aggressive treatment of the underlying plasma cell disorder, survival is poor. With cardiac involvement, median survival is about 4 months.
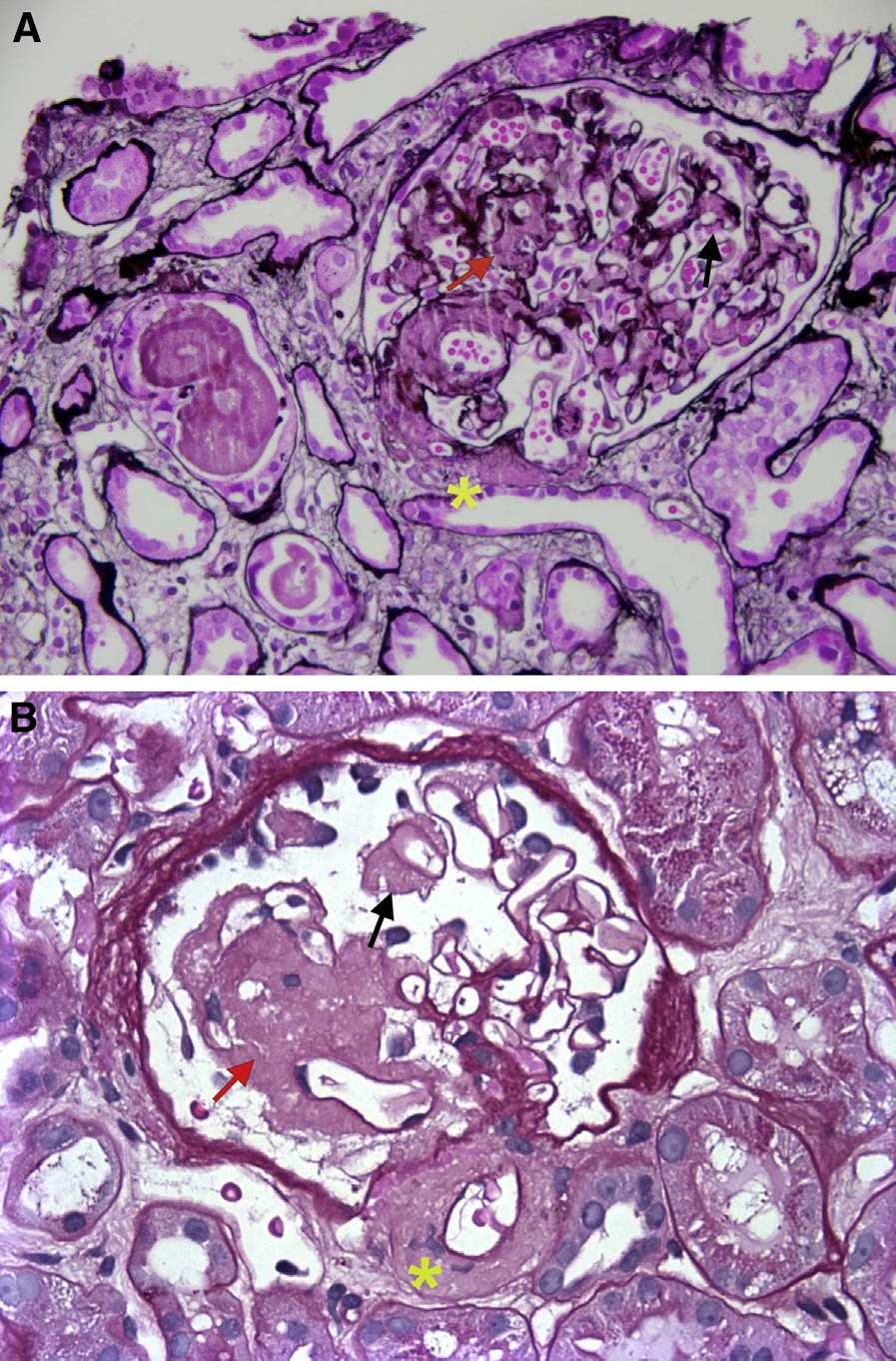
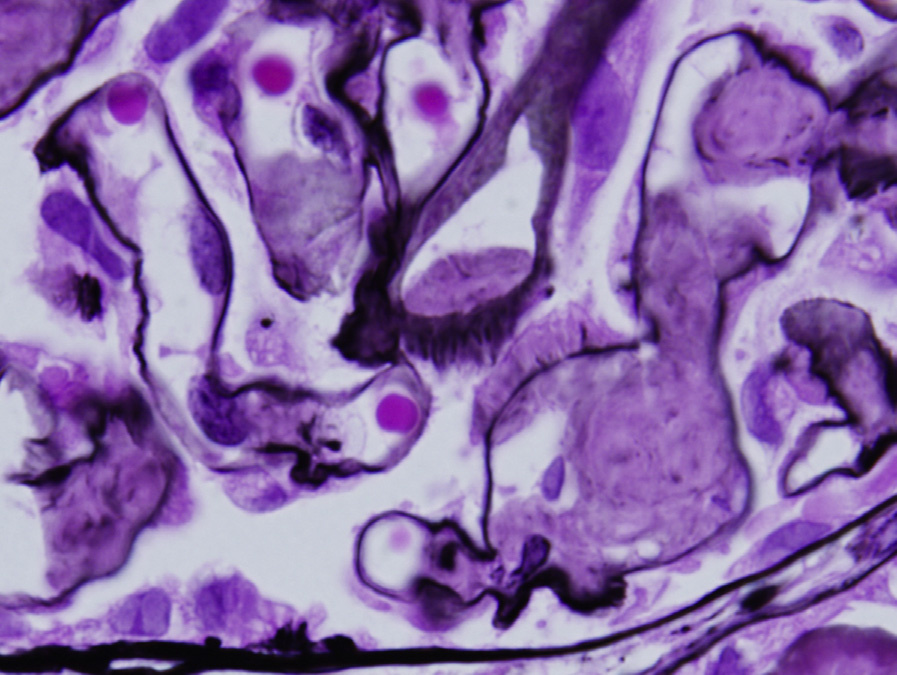
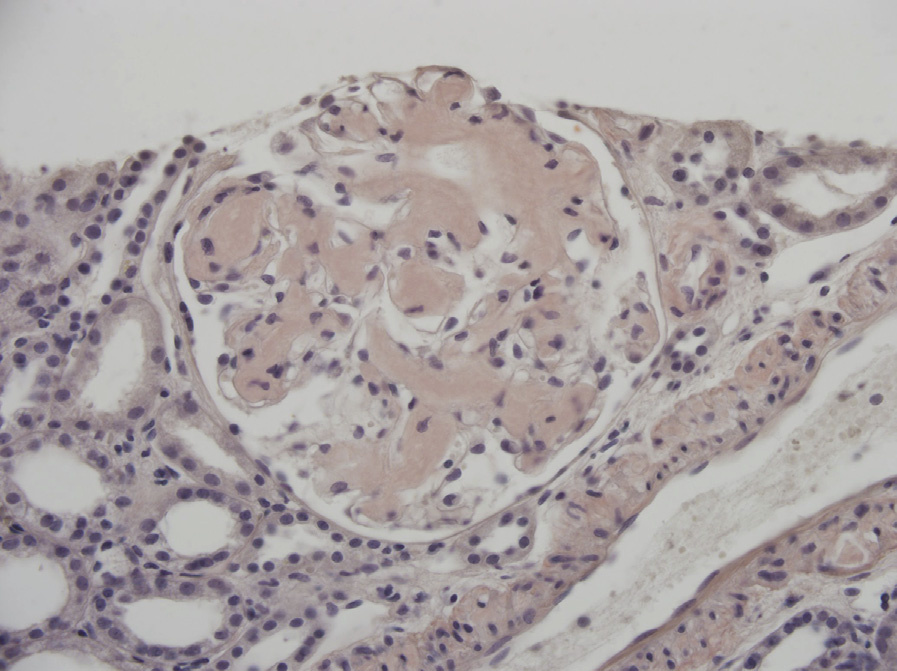
Light microscopy: Amyloid deposits involve the mesangium as acellular, amorphous, silver-negative, pale pink, cotton candy–like material. Amyloid involving the glomerular basement membranes (GBMs) results in segmental, long, feathery, silver-positive spikes. Arterioles and arteries often also show amyloid deposits.
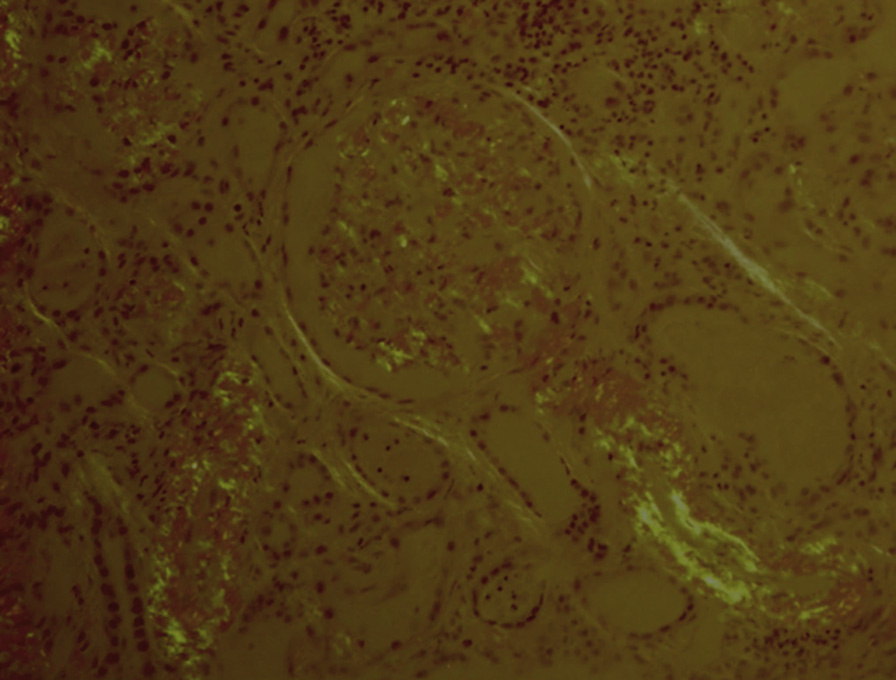
Interstitial amyloid has a similar pale-pink, acellular appearance. Diagnosis is by Congo red positivity, with apple-green birefringence under polarized light.
IF microscopy: Smudgy mesangial deposits, some extending to irregular capillary wall, arterioles, arteries, and interstitium depending on the extent of amyloid, stain in monoclonal pattern for one light chain. λ light chain most commonly gives rise to amyloid deposits. Very rare cases of heavy chain amyloid have been described.
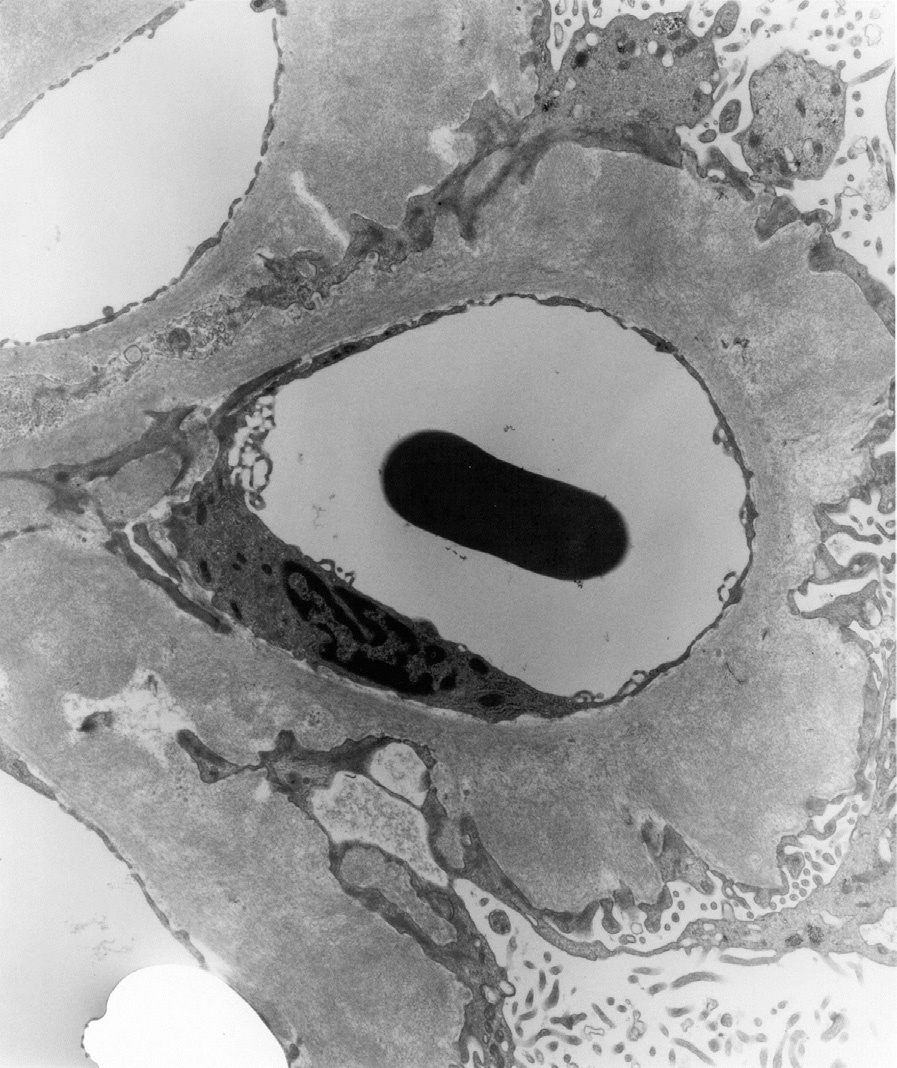
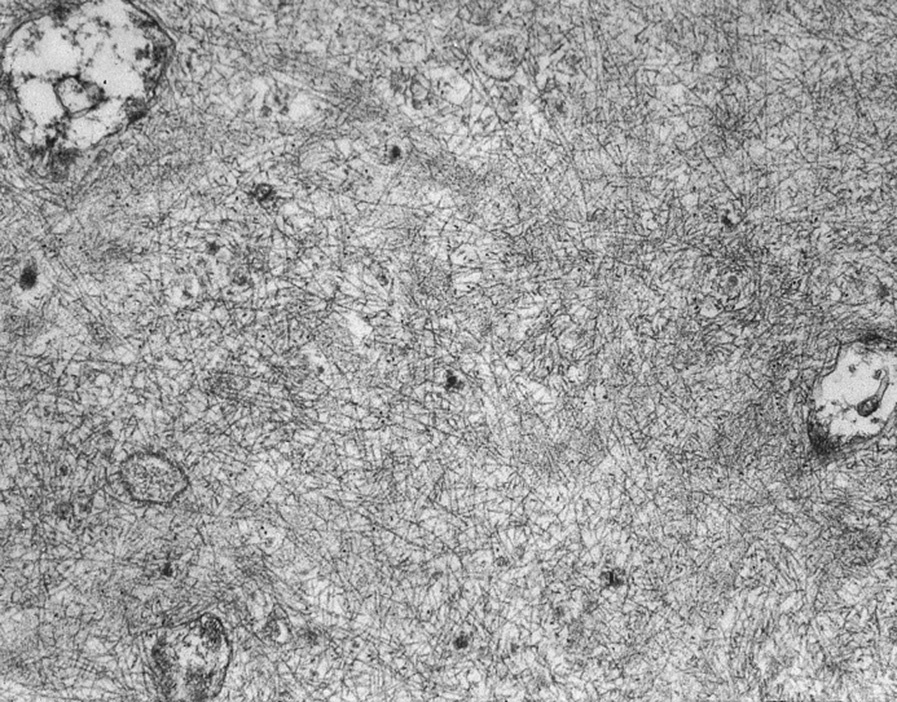
Electron microscopy (EM): Mesangial deposits of extracellular, randomly arranged, straight fibrils 9-11 nm in diameter are seen in the mesangium, and may also involve GBMs with extensive foot process effacement.
AL amyloid is due to deposition of a monoclonal light chain that has formed a beta-pleated sheet, which accounts for the Congo red intercalation and apple-green appearance. Beta-pleats resist proteolysis, and progressive amyloid deposition results in organ dysfunction. The monoclonal protein is due to underlying plasma cell dyscrasia, with or without the patient meeting criteria for multiple myeloma by bone marrow examination. Patients with renal AL amyloidosis without diagnostic multiple myeloma were previously said to have monoclonal gammopathy of undetermined significance, now called monoclonal gammopathy of renal significance.
AL amyloid may be distinguished from other causes of mesangial expansion by specific light chain staining, positive Congo red staining, and fibrils on EM.
Fibrillary glomerulonephritis is Congo red negative, with polyclonal IgG and proliferative appearance; diabetic nephropathy shows no deposits; other monoclonal immunoglobulin deposition diseases are Congo red negative, with absence of amyloid fibrils on EM. Other causes of membranoproliferative glomerulonephritis pattern show disease-specific IF and EM appearances.