Microscopy Images
Cryoglobulinemic glomerulonephritis (GN) is caused by intracapillary, capillary wall (often subendothelial), and mesangial cryoglobulin deposits, giving a membranoproliferative pattern of injury. Patients have nephritic/nephrotic syndrome with various levels of kidney function. Purpura and arthralgia occur in about one-third, with vasculitis affecting skin and kidneys less commonly. Abnormal serologic studies include low C4 in three-quarters and low C3 in half. All 3 types of cryoglobulins, including those due to both monoclonal and polyclonal immunoglobulins, can cause cryoglobulinemic GN, although most commonly it occurs in settings of type II (“mixed”) cryoglobulinemia secondary to hepatitis C virus (HCV) infection. Most patients with type II or III cryoglobulins have a positive rheumatoid factor. Novel antivirals may effectively treat HCV and the associated cryoglobulinemia, with beneficial effects on the kidney disease. However, mortality remains substantial: ~50% 10-year survival in those with mixed cryoglobulinemia and decreased kidney function at presentation. Cryoglobulinemic GN can recur in the transplant.
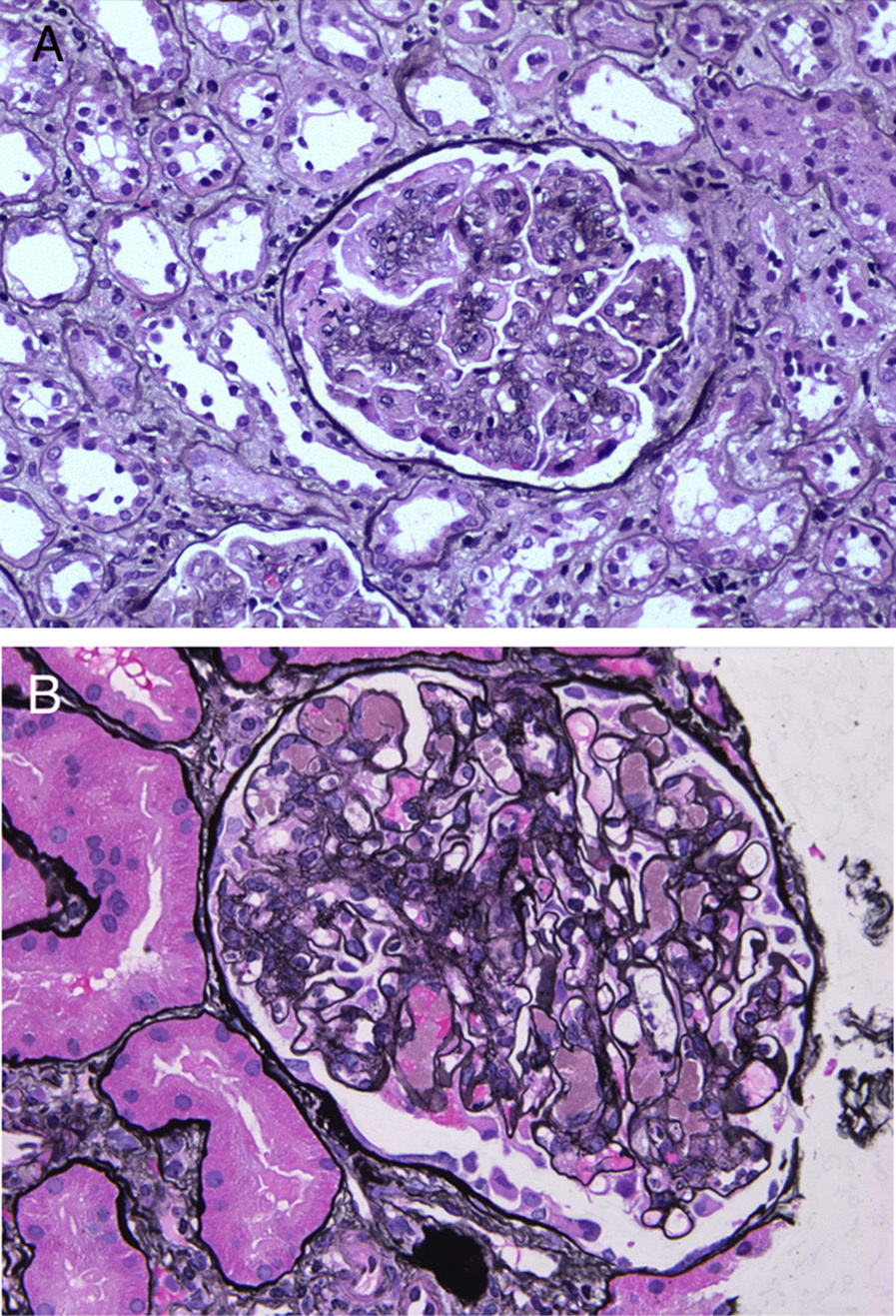
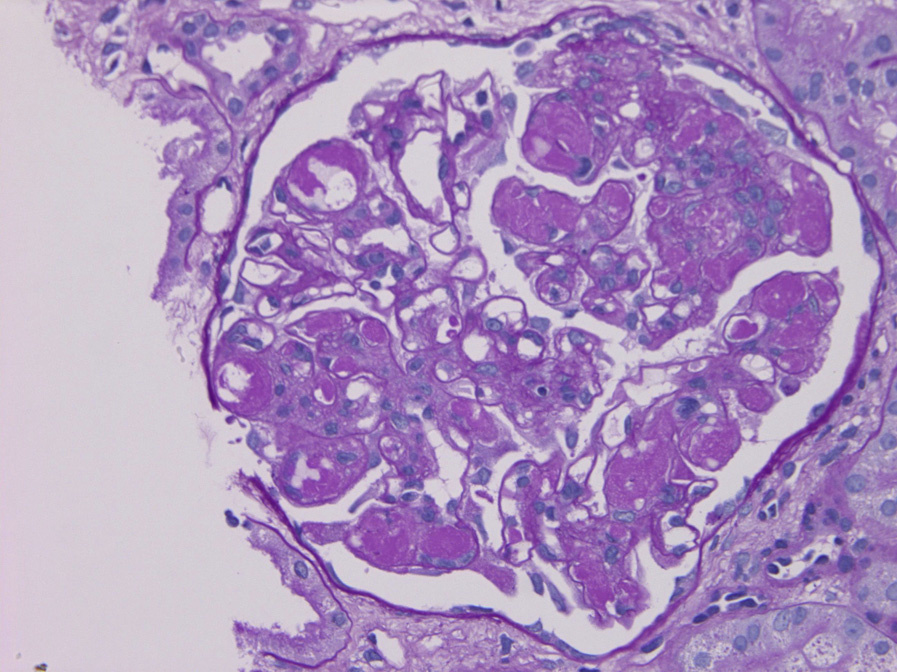
Light microscopy: There is mesangial proliferation and often diffuse and global endocapillary hypercellularity. Eosinophilic refractile intracapillary “cryoplugs” that are strongly periodic acid–Schiff (PAS) positive are due to the IgM component of these deposits.
The acute phase has frequent neutrophils, with increased monocyte/macrophages in both acute and chronic stages. Arterioles and small arteries may show leukocytoclastic vasculitis, sometimes with cryoglobulin deposits. Crescents may be present.
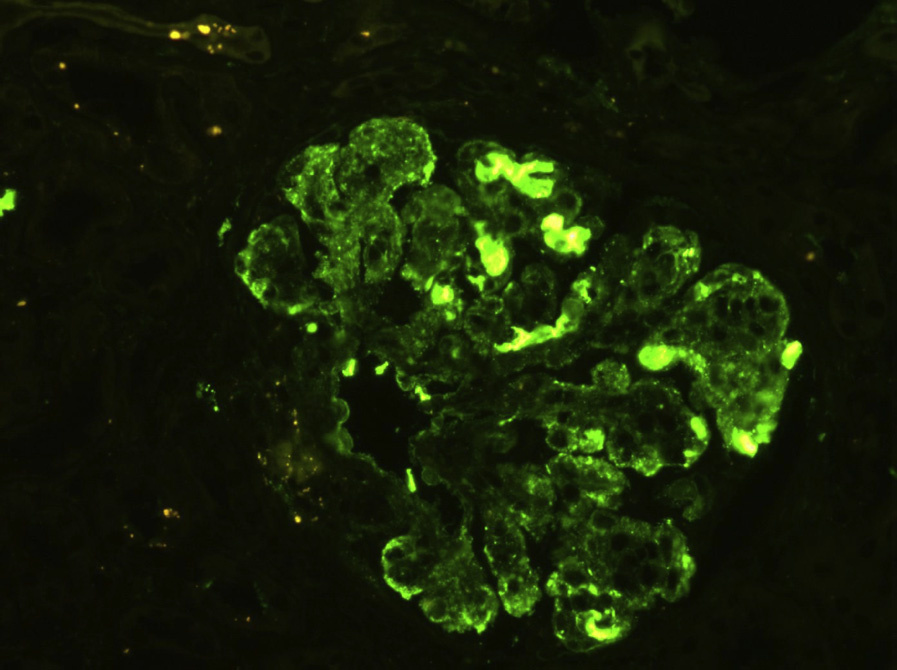
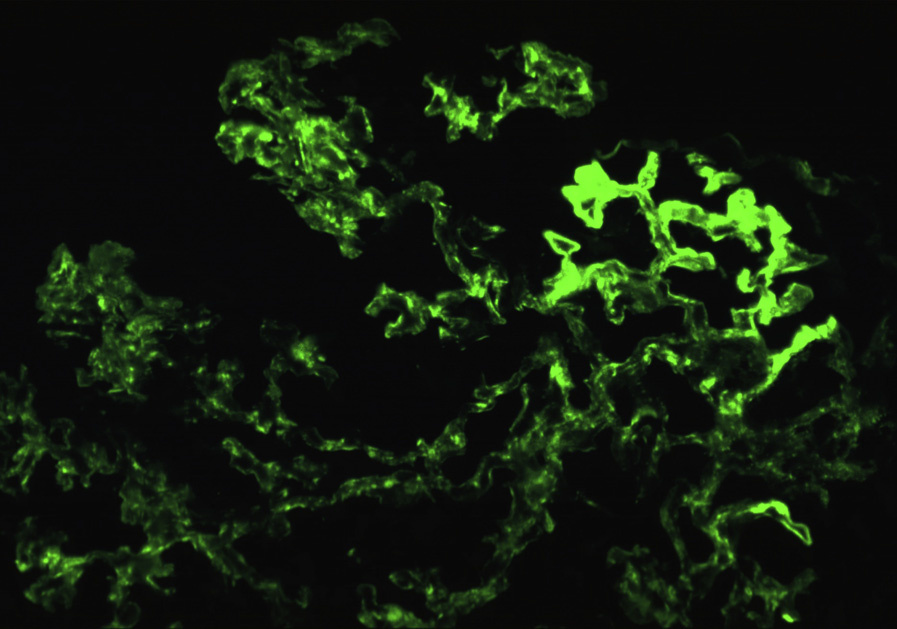
Immunofluorescence (IF) microscopy: Mesangial and chunky irregular capillary wall deposits often appear sausage-shaped due to molding under the glomerular basement membrane (GBM). There is prominent IgM and C3, often with clonal bias of κ light chain versus λ, with similar or lesser amounts of IgG or C1q. Cryo-plugs typically show strong IgM and clonal κ or λ staining, and may show similar staining for IgG in type II and III cryoglobulinemia.
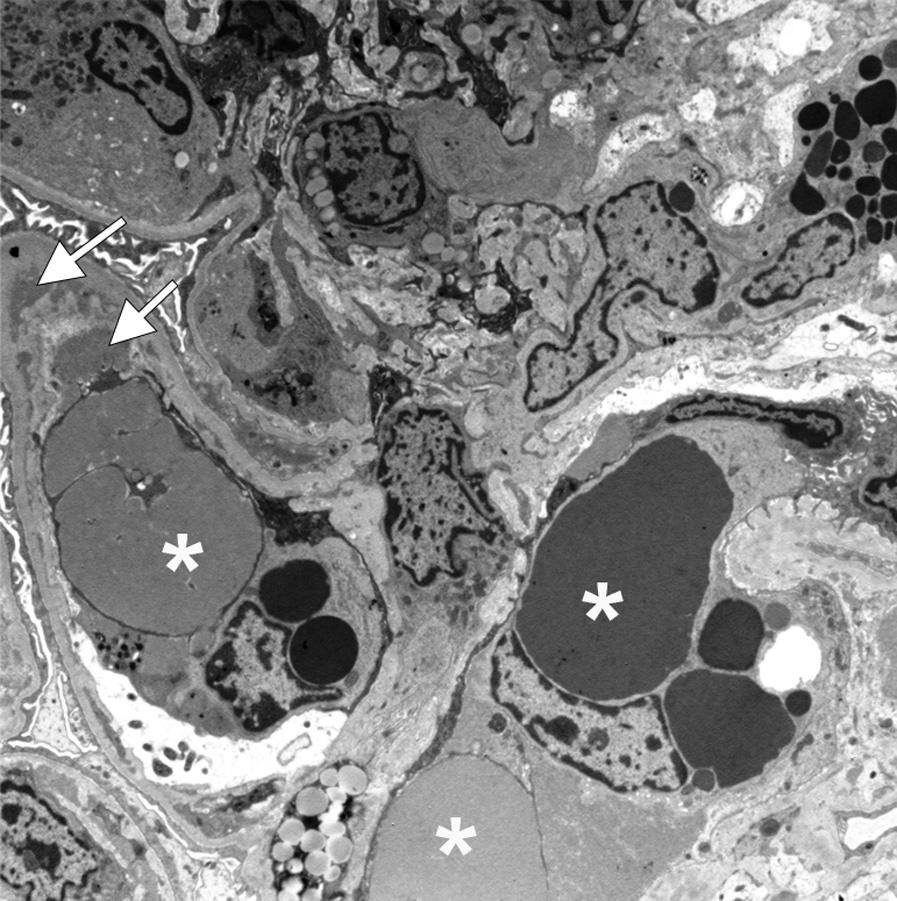
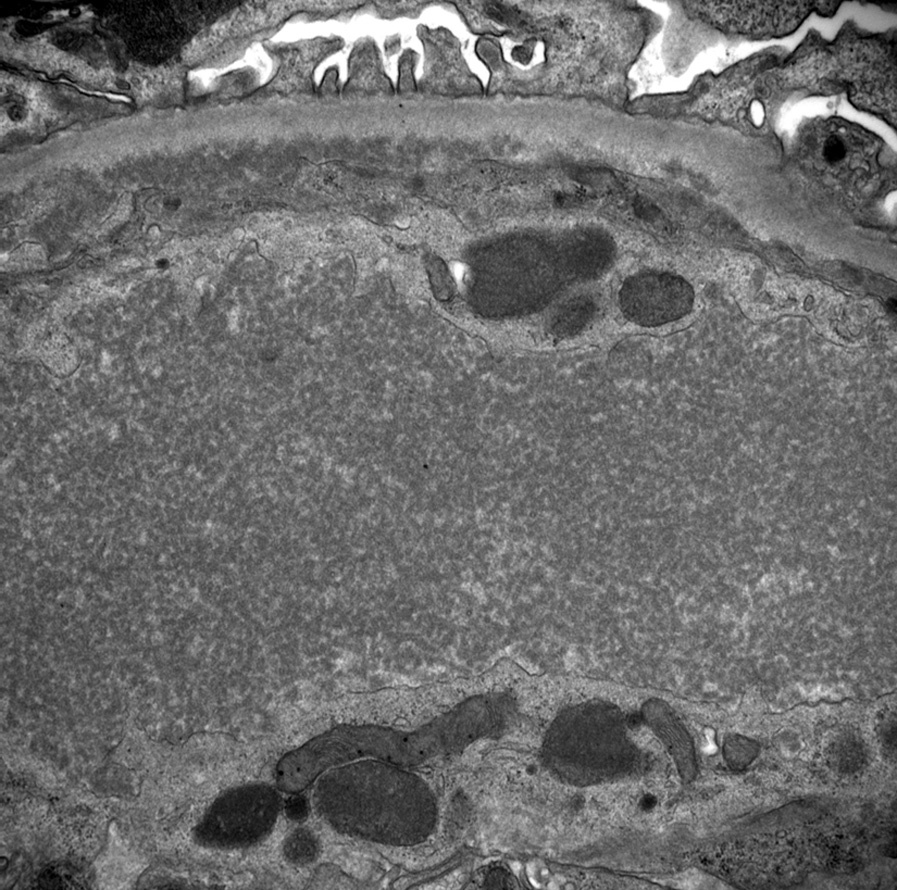
Electron microscopy (EM): Mesangial and subendothelial deposits, often with interposed cells and double contours due to new GBM formation beneath subendothelial deposits are common. Intracapillary deposits, extensive foot process effacement, and endocapillary hypercellularity also occur. Deposits may show vague, short fibrillary substructure and be organized as tactoids similar to fibrin. Monoclonal cryoglobulin deposits may be microtubular and highly organized.
Mixed cryoglobulinemia is most commonly caused by HCV, with some cases caused by lymphoproliferative or autoimmune disorders. Most patients show an membranoproliferative GN (MPGN) pattern of injury in response to the subendothelial deposits.
Distinguishing features of MPGN due to other causes are as follows: fibrillary GN (polyclonal IgG, randomly arranged fibrils by EM), amyloid (more acellular, typical fibrils by EM, Congo Red positive), C3 glomerulopathies (C3 with no or minimal immunoglobulin by IF, dense deposits and dense deposit disease), proliferative GN with monoclonal deposits (monoclonal immunoglobulins by IF), and diffuse lupus nephritis (full-house [IgG, IgA, IgM, C3, C1q] IF staining, endothelial tubuloreticular aggregates by EM). Immunotactoid glomerulopathy appears as welldefined, long microtubular deposits, often in parallel arrays, without detectable cryoglobulins, and more typically is IgG dominant.