Microscopy Images
The transplant may be affected by numerous processes that culminate in scarring of all compartments of the kidney. These changes were previously referred to as chronic allograft nephropathy (CAN), to convey the presence of scarring from any cause. In 2005, the Banff working group of transplant pathology introduced the term interstitial fibrosis/tubular atrophy (IF/TA), to emphasize that no etiology is assigned when this diagnosis is made. Patients may be of any age. IF/TA typically develops months or even years after transplantation. Patients present with slowly increasing serum creatinine, with variable proteinuria, depending upon the severity of the injury, and if it is accompanied by glomerular scarring. When specific etiologies of IF/TA can be discerned, they should be described. IF/TA can result in graft failure if underlying causes are not identified and specifically treated.
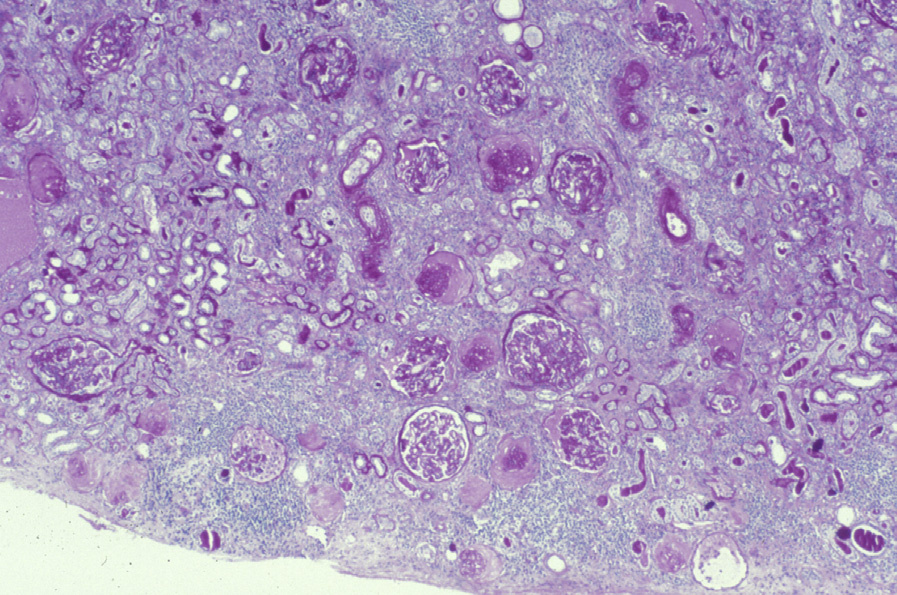
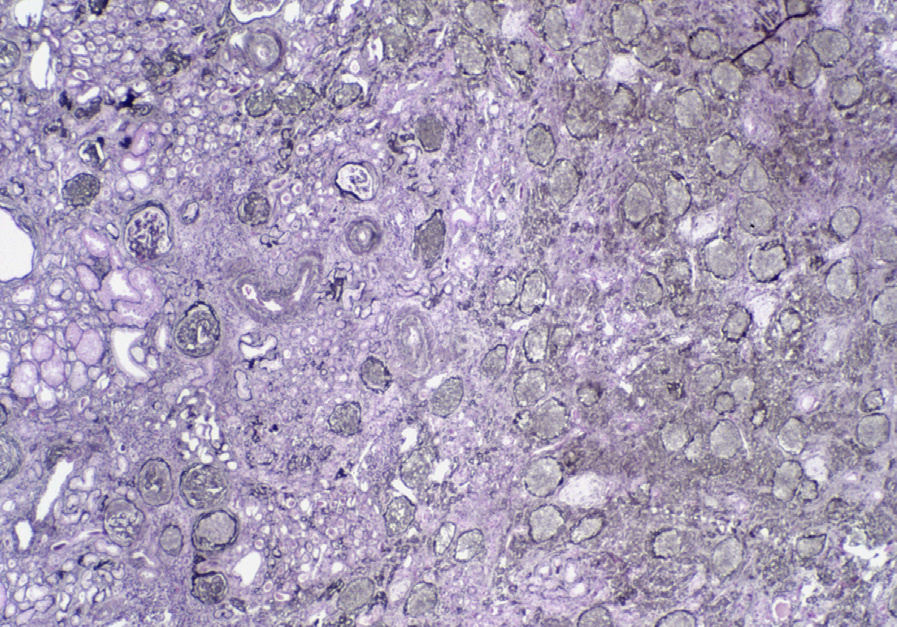
Light microscopy: There is proportional interstitial fibrosis and tubular atrophy in a diffuse distribution.
Glomeruli may show ischemic changes with corrugation of basement membranes and thickening of capillary walls with accompanying segmental and/or global glomerulosclerosis.
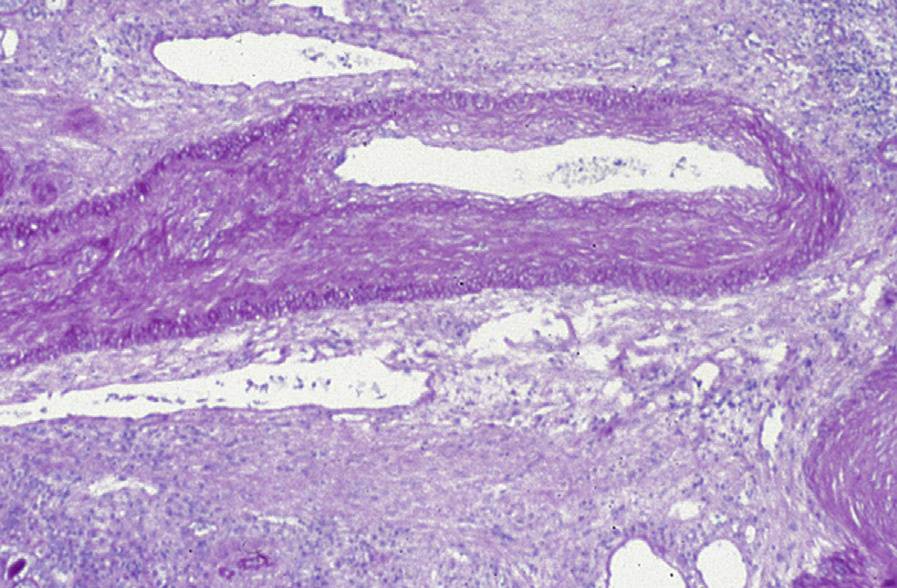
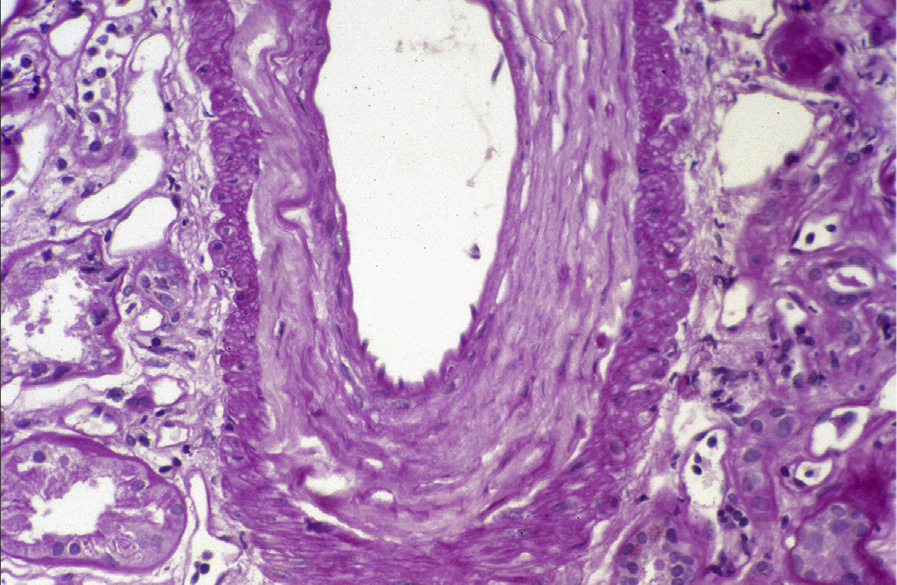
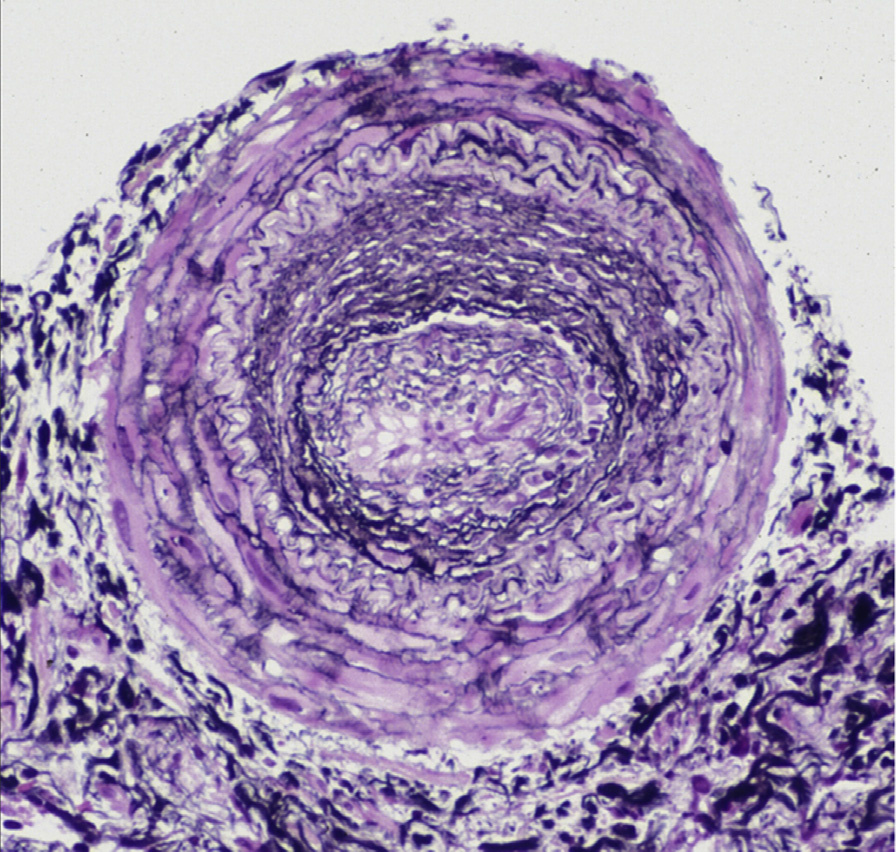
Severity is graded depending upon whether it involves ≤25% of cortical area (grade 1, IF1/TA1), 26%-50% (grade 2, IF2/TA2), or >50% (grade 3, IF3/TA3). Vascular lesions include arteriolar and arterial sclerosis with intimal proliferation and medial hypertrophy, and are scored by Banff criteria from 0-3, representing no narrowing of the lumen, or ≤25%, 26%-50%, or >50%, respectively.
Immunofluorescence microscopy: No specific changes.
Electron microscopy: Glomeruli not involved by sclerosis do not show specific changes. In sclerosed glomeruli, there is variable foot process effacement.
Scarring of the transplant may occur due to many underlying injuries, including hypertension, calcineurin inhibitor (CNI) toxicity, chronic pyelonephritis, reflux and/or obstruction, viral infections, diabetic kidney disease, crystals (eg, calcium phosphate), or recurrence of disease or de novo injuries. Each of these has specific morphologic findings discussed in detail elsewhere. When specific causes have been eliminated, the term IF/TA, also previously called CAN, is used. Of note, this term does not cover glomerular or vascular changes, which should be described separately.
Specific causes of fibrosis and atrophy that should be considered and diagnosed include chronic CNI toxicity, with its classical striped interstitial fibrosis; chronic antibody-mediated rejection (CAMR), with concentric intimal fibrosis of arteries and transplant glomerulopathy with characteristic double contours of the glomerular capillary basement membranes, often with positive C4d in peritubular capillaries; chronic pyelonephritis or reflux nephropathy with characteristic jigsaw pattern scarring; obstruction with dilatation of tubules and Bowman’s spaces; and viral infection with characteristic viral cytopathic changes. CAMR is distinguished from nonspecific IF/TA (CAN) changes by the presence of transplant glomerulopathy, multiple (>7) layering of peritubular capillary basement membranes, intimal fibrosis of arteries but without duplication of the internal elastica (as would be seen with hypertension), and may also show persistent glomerulitis and peritubular capillaritis.