Microscopy Images
Acute uncomplicated pyelonephritis is most commonly due to bacterial infection ascending from the lower urinary tract, and occurs more often in young adult women, 15 to 29 years old, who are sexually active; this is on account of the shorter urethra in women and its potential contamination with intestinal bacteria. As discussed in the following, complicated acute pyelonephritis has predisposing findings. The incidence is estimated to be 15 to 17 cases per 10,000 women, contrasting 3 to 4 cases per 10,000 men. Patients most often have flank pain and dysuria with tenderness and fever. Urinalysis shows pyuria, often with white blood cell casts and microscopic hematuria, with positive urine cultures. Unilateral acute pyelonephritis does not result in GFR loss. Uncomplicated pyelonephritis has an excellent prognosis when treated. Complicated acute pyelonephritis may not respond as well to therapy, with frequent recurrence and predilection to chronic pyelonephritis.
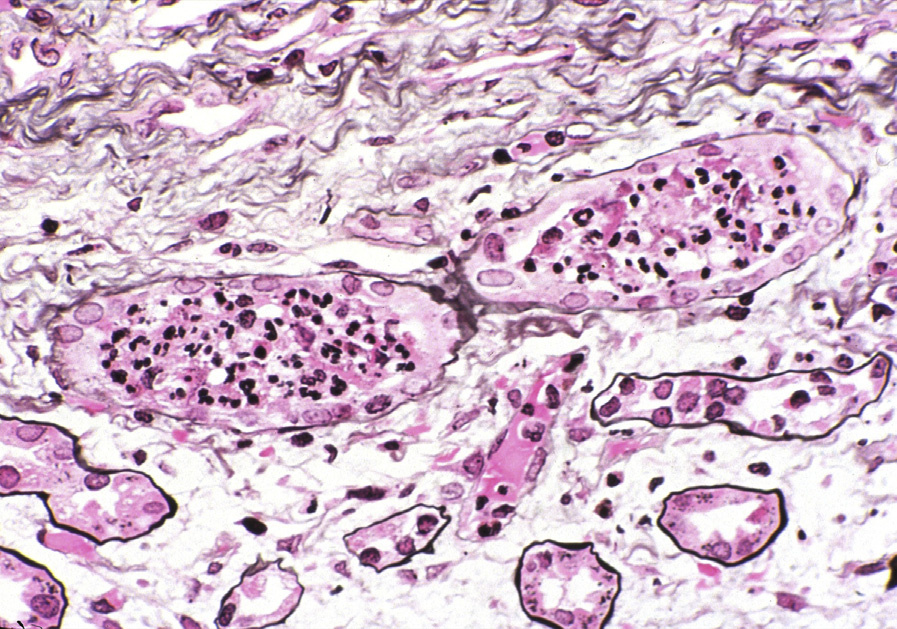
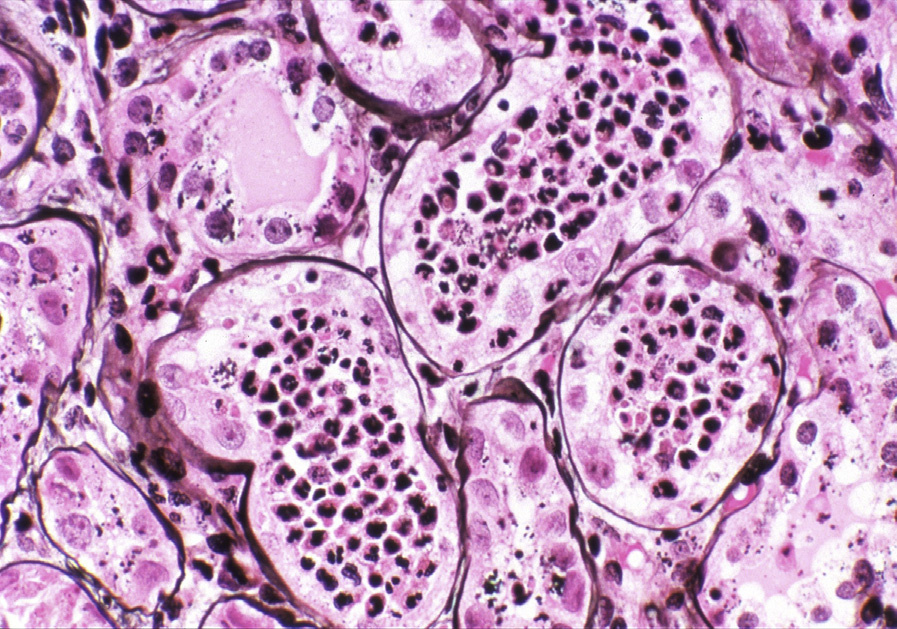
Light microscopy: There is marked inflammatory infiltrate with dominant neutrophils, forming plugs within tubules, and extending to the interstitium, occasionally with tubular destruction and microabscesses.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: No specific findings.
Acute pyelonephritis is most often due to ascending infection, and therefore commonly occurs secondary to cystitis. The most frequent organism is E. coli.
Complicated acute pyelonephritis occurs due to underlying factors. In infants, abnormalities of the urinary tract may be responsible; at any age, but most often in older patients, causes include diabetes, decreased immunity, obstruction, and stones. Occasionally there may be a hematogenous route of infection, in which case the microabscesses are more widespread and typically bilateral. P. fimbriae, a mannose-resistant adhesin of uropathogenic E. coli, mediate adhesion to the urothelium. Variants of genes involved in the antimicrobial defense of the urothelium have also been postulated as risk factors for recurrent urinary tract infections, including acute pyelonephritis.
Acute pyelonephritis due to bacteria has identical morphology regardless of which bacteria is causal.
Some viral infections, particularly hantavirus or adenovirus, may show interstitial inflammation and hemorrhage, but tend to have predominant mononuclear cells, with viral cytopathic changes. Acute tubulointerstitial nephritis due to hypersensitivity injury does not have prominent neutrophils, but rather dominant lymphocytes with scattered plasma cells and may have frequent eosinophils. Early light chain cast nephropathy may have a neutrophil reaction to the casts, and diagnosis is made by monoclonal staining of casts.