Microscopy Images
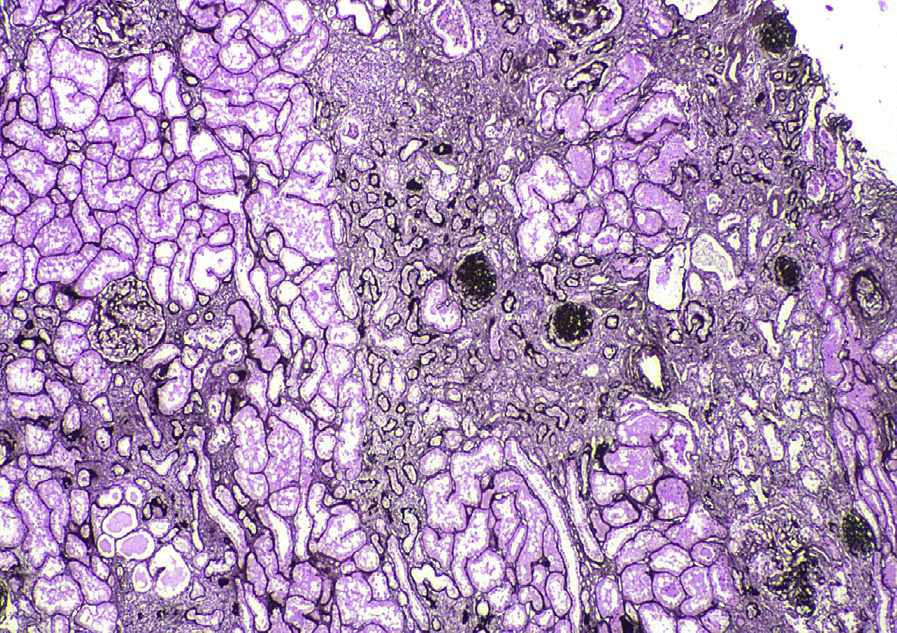
![Chronic pyelonephritis with geographic scarring and thyroidization of tubules (low [A] and high [B] power magnification; periodic acid–Schiff stain).](../assets/Chronic_Pyelonephritis_004.jpg)
Chronic pyelonephritis occurs in patients at risk for repeated bouts of acute pyelonephritis, and is thus most often the result of complicated acute pyelonephritis. However, not all have preceding overt signs of acute pyelonephritis, such as fever, malaise, or flank pain. Patients present with nonspecific signs of chronic kidney disease. Urinalysis typically shows pyuria, often with microscopic hematuria, occasionally white blood cell casts and positive urine cultures.
Chronic pyelonephritis due to structural abnormalities occurs more often in infants and children younger than 2 years. About 5% to 6% of children with chronic pyelonephritis due to vesicoureteral reflux develop long-term complications such as hypertension, and around 2% may progress to kidney failure.
Conversely, chronic pyelonephritis may cause as much as 20% of end-stage renal disease occurring in children. In adults, diabetes, immunocompromise, nephrolithiasis, obstruction, reflux, or neurogenic bladder may lead to chronic pyelonephritis. When chronic pyelonephritis is bilateral, chronic kidney disease often ensues.
Light microscopy: There is patchy tubulointerstitial scarring in a so-called geographic or jigsaw pattern with well-delineated, irregular areas of scarring due to the patchy initial infection from the ascending route.
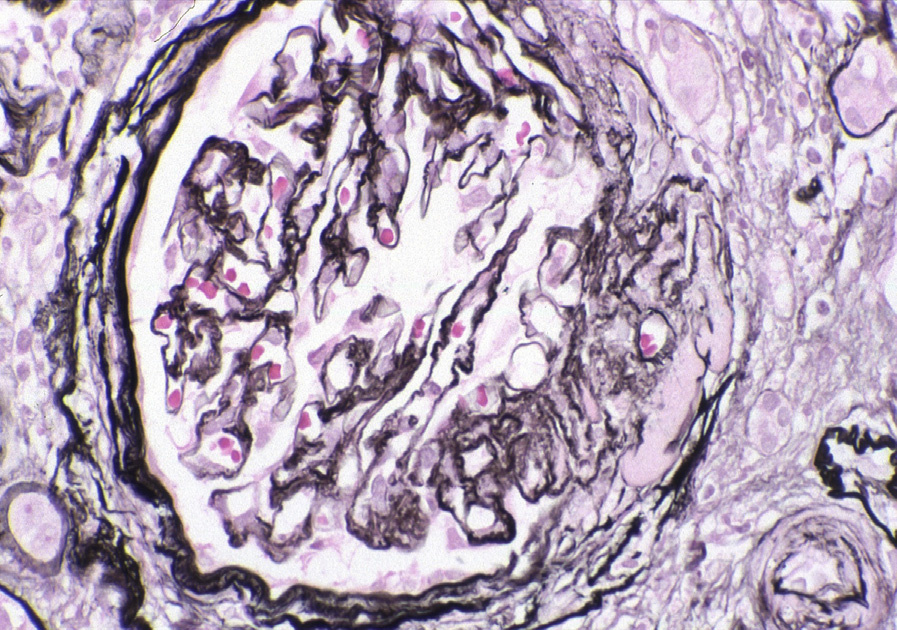
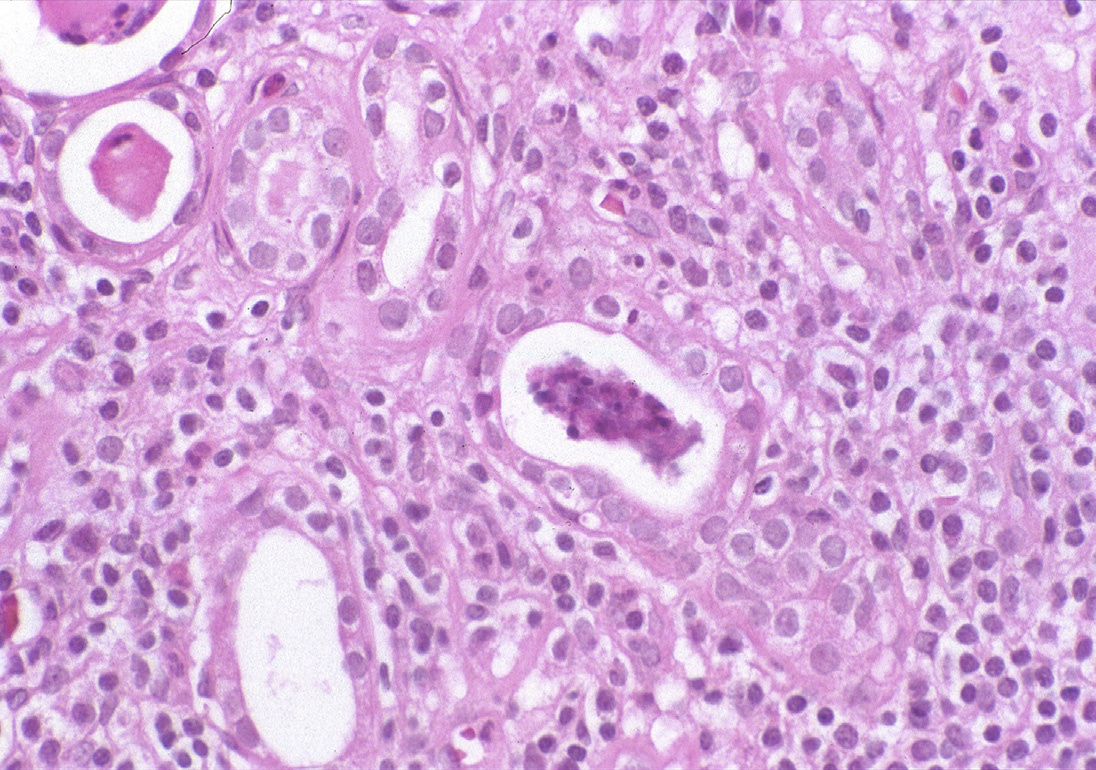
There is accompanying thyroidization of tubules (ie, atrophic tubules filled with casts that resemble thyroid colloid), interstitial lymphoplasmacytic infiltrate, and often periglomerular fibrosis and secondary segmental glomerulosclerosis.
Immunofluorescence microscopy: No specific staining.
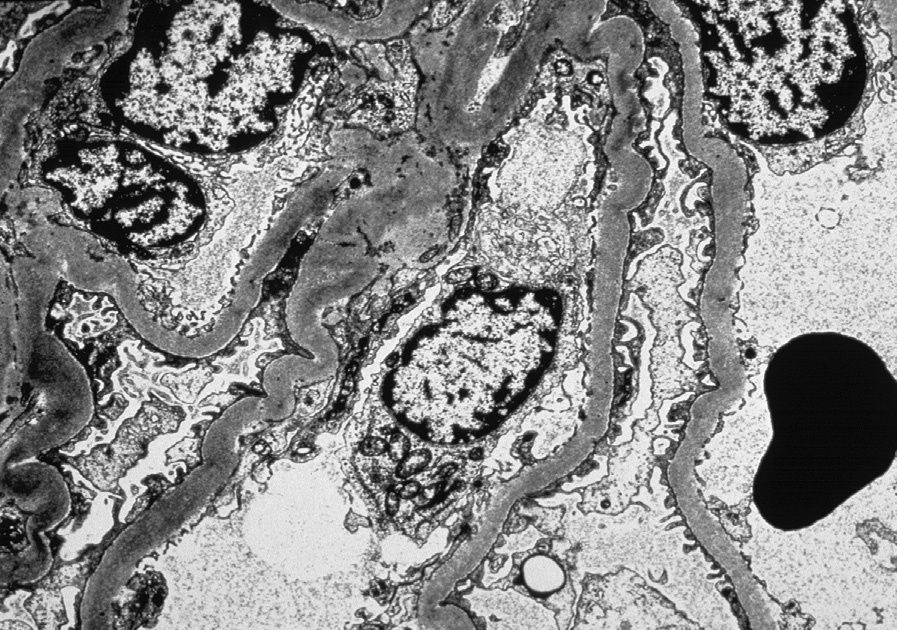
Electron microscopy: Segmentally scarred glomeruli show variable foot process effacement, whereas uninvolved glomeruli do not show specific changes.
Chronic pyelonephritis is a consequence of repeated or untreated acute pyelonephritis. The underlying etiology thus is most often structural abnormalities such as congenital abnormalities of the kidney and urinary tract, seen in children, which may be unilateral or bilateral, or acquired obstruction such as that seen with stones, prostatic hypertrophy, lymphadenopathy or retroperitoneal fibrosis, or neurogenic bladder. E. coli remains the most common etiologic agent, as in acute pyelonephritis.
Scarring of the tubules, interstitium, and secondary glomerular scarring may also occur in hypertension-associated injury, reflux nephropathy without bacterial infection, and due to any other cause of chronic tubulointerstitial nephritis. The presence of sharply delineated, geographic scarring suggests chronic pyelonephritis/reflux nephropathy.
Xanthogranulomatous pyelonephritis has marked foam cells, and is more often associated with kidney stones and obstruction, most commonly with Proteus infection. Malakoplakia is characterized by foamy macrophage inflammation and Michaelis-Gutmann bodies (the consequence of incompletely digested bacteria).