Microscopy Images
Tubular atrophy is a general term that describes several patterns of chronic tubular injury with thickened tubular basement membranes, and clinically manifests as chronic kidney disease with decreased glomerular filtration rate. Increased extent of tubular atrophy and accompanying interstitial fibrosis correlates with worse prognosis. Proteinuria is variable, depending on cause.
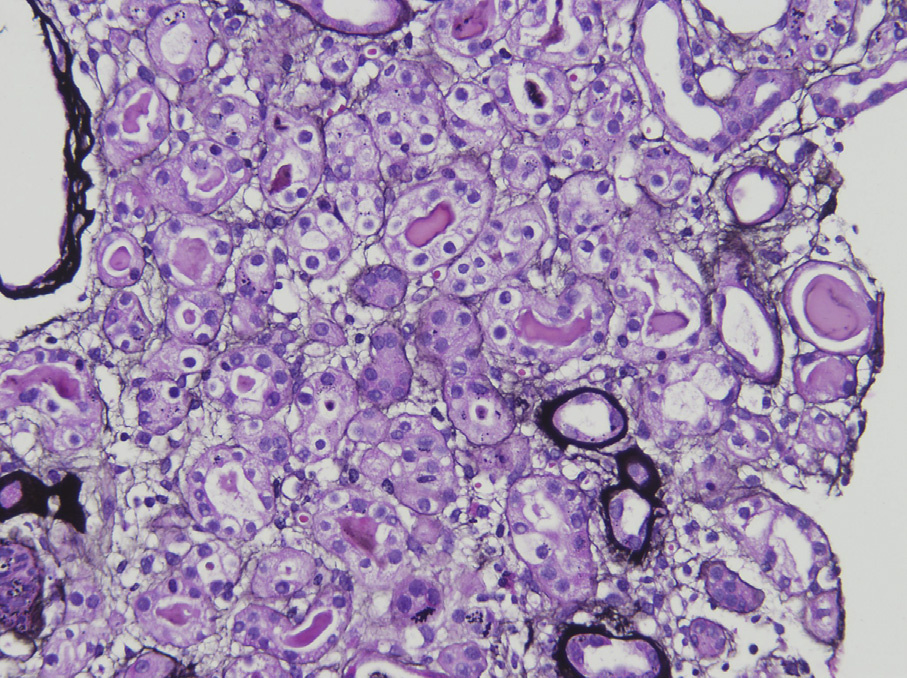
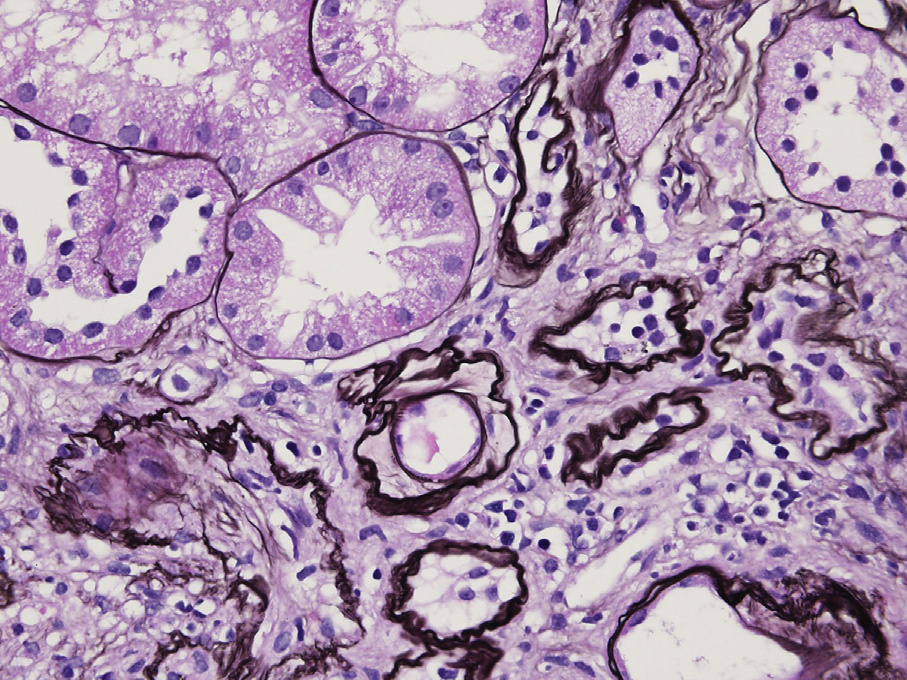
Light microscopy: The most common pattern, not otherwise specified, shows thickened and wrinkled tubular basement membranes with flattened, simplified tubular epithelial cells and contraction of the tubular lumen. There is a proportional extent of interstitial fibrosis separating tubular profiles. The endocrinization pattern is characterized by shrunken tubules with cuboidal epithelial cells with narrowed lumen and little to no thickening of tubular basement membranes.
Thyroidization of tubules is characterized by enlarged round tubules with markedly flattened epithelium with uniform intratubular casts, resembling thyroid colloid.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: Thickened, often lamellated tubular basement membranes with simplified tubular epithelial cells.
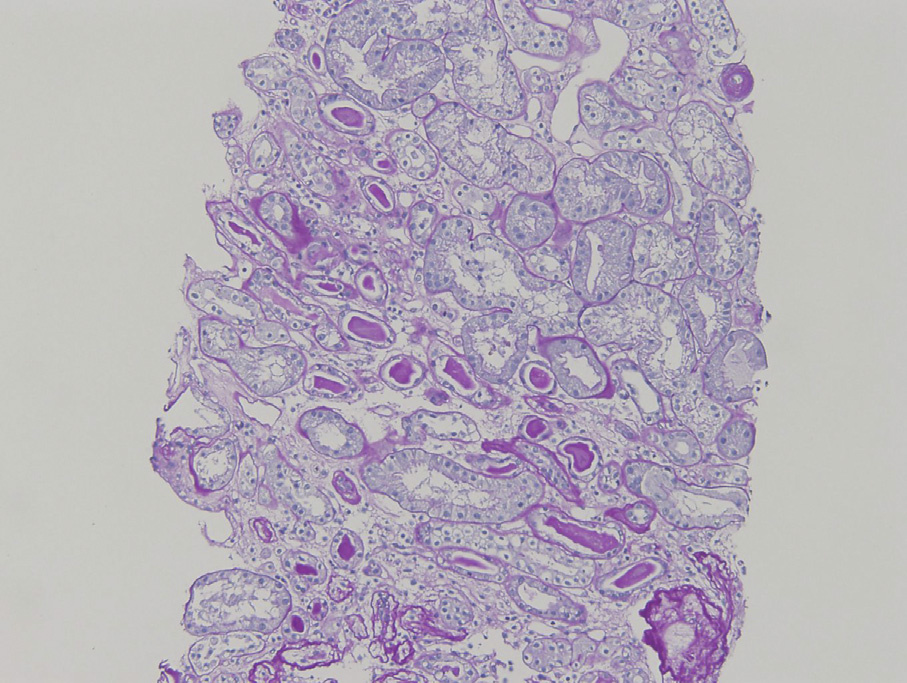
Tubular atrophy of usual type is caused by any chronic injury of glomerular, vascular, interstitial, or tubular origin. The endocrinization pattern of tubular atrophy can be associated with stenosis of the renal artery or its major branches. The thyroidization pattern commonly occurs with injury related to urinary reflux or chronic pyelonephritis, and is then often present in a sharply delineated “jigsaw” pattern demarcating normal and atrophic regions. On the other hand, sharply delineated wide areas of tubular atrophy and interstitial fibrosis with straight borders demarcating normal and atrophic regions can suggest a vascular insult (such as stenosis or past thrombi). Chronic ischemia in conditions affecting smaller arteries (such as hypertension or chronic calcineurin inhibitor toxicity) creates tubular atrophy and interstitial fibrosis along the medullary rays, creating a striped pattern of scarring.
Atrophic tubules must be distinguished from acute tubular injury as both can show extensive tubular epithelial changes. In acute tubular injury, tubules are often dilated and tubular basement membranes are smooth and maintain normal thickness, in contrast to the contracted tubules with thickened and wrinkled tubular basement membranes of tubular atrophy. Further, in acute tubular injury, tubules are usually back-to-back or mildly separated by interstitial edema, while in tubular atrophy tubules can be separated by interstitial fibrosis.
Uniform thickening of tubular basement membranes without shrinkage and otherwise healthy epithelial cells can be seen in diabetic nephropathy. Duplication, or lamellation, thickening, and disruption of tubular basement membranes with tubular dilatation can be seen in medullary cystic kidney disease/nephronophthisis.
Typical imaging findings and genetic testing can differentiate these conditions, if clinically suspected.