Microscopy Images
Anti-GBM antibody–mediated glomerulonephritis usually presents with rapidly progressive glomerulonephritis. In some patients, the antibody cross-reacts with alveolar basement membranes, and about half also have hemoptysis due to lung involvement. This constellation of kidney and lung disease is called Goodpasture syndrome. The incidence in the United States is about one per million per year. Patients show a bimodal age distribution (peaks at the late teens to age 20, and at 50-70 years old), with equal distribution by sex. About a quarter of patients also have positive ANCA, usually myeloperoxidase (MPO)-ANCA with corresponding additional clinical features of microscopic polyangiitis. Disease usually follows a one-hit course, without relapses and remissions. In patients with initial serum creatinine <5.7 mg/dL, kidney and patient prognosis are excellent with aggressive treatment; those with higher creatinine or requiring dialysis at presentation have very poor kidney survival, with about one-third dying within one year. Patients with combined anti-GBM disease and ANCA typically have a clinical course dominated by anti-GBM disease and accordingly poor prognosis.
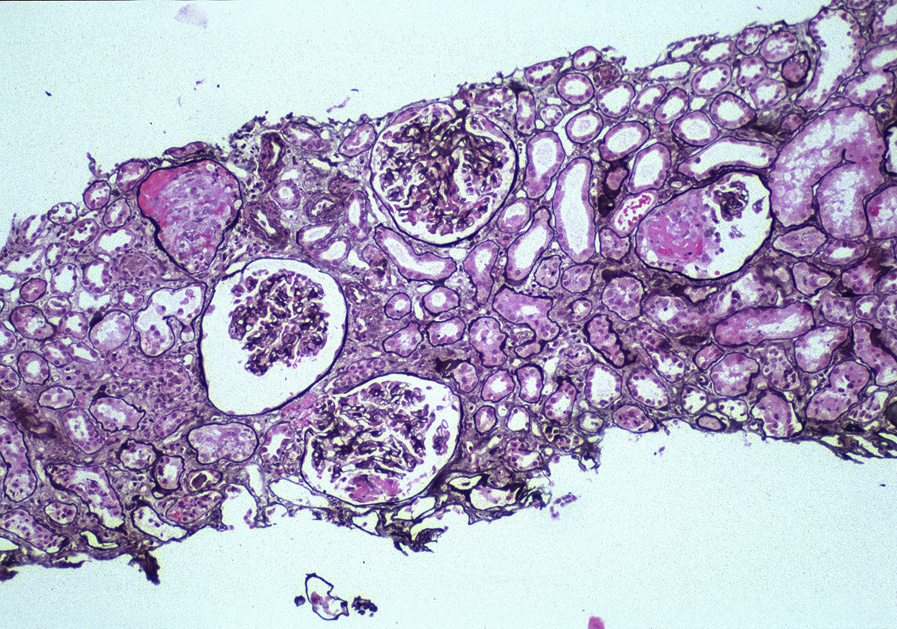
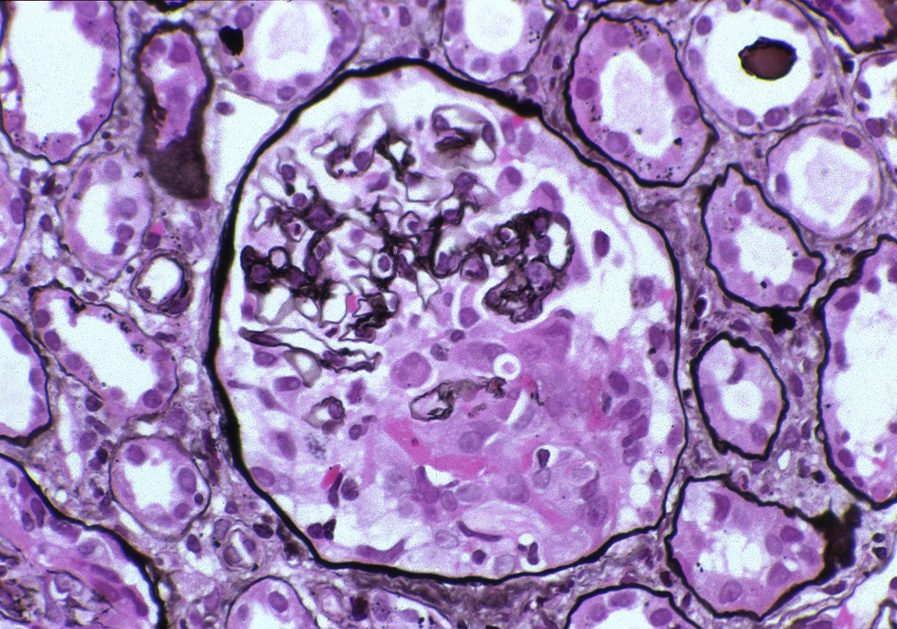
Light microscopy: There are breaks of the GBM due to fibrinoid necrosis, with resulting crescents.
Crescents typically are widespread at diagnosis, involving most glomeruli. Uninvolved segments of glomeruli do not show proliferative lesions. All crescents tend to show the same stage of activity and chronicity, reflecting the disease’s one-hit nature. There may be surrounding inflammation, occasionally granulomatous, around glomeruli with disrupted Bowman capsule. Extraglomerular renal involvement by vasculitic lesions is limited to patients with concomitant ANCA.
Tubular injury, RBC casts, and interstitial inflammation occur proportionally to the degree of crescents.
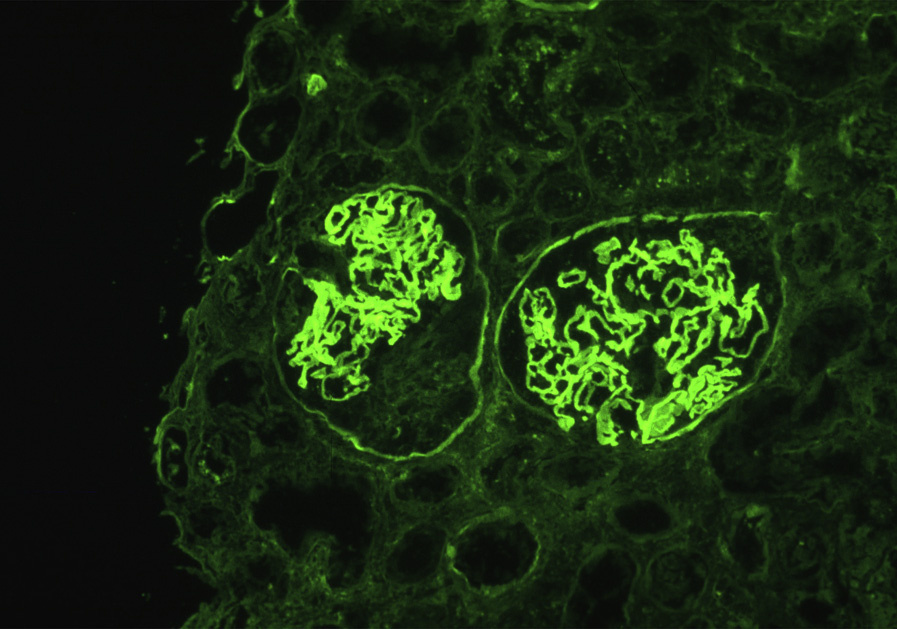
Immunofluorescence microscopy: There is strong linear GBM staining for polyclonal IgG. C3 is positive in most cases, weaker than IgG, with a discontinuous or occasional granular pattern. Rare cases have IgA or IgM linear staining with apparent antiGBM antibody–mediated disease. Tubular basement membrane staining may also be present due to cross-reactivity of the antibody.
Electron microscopy: No deposits are detected.
GBM breaks with necrosis and crescent formation are observed.
Autoantibodies against the NC1 domain of the α3 chain of type IV collagen cause anti-GBM antibody–mediated glomerulonephritis. This antibody also can cross-react with alveolar basement membranes, giving rise to Goodpasture syndrome with combined kidney and lung lesions. The autoantibody is due to a conformational change in the α3 (IV) collagen. Preceding and possibly inciting events include upper respiratory infection or exposure to solvents or toxic aerosols. In some patients, membranous nephropathy, or preceding ANCA-related injury, can be a trigger. If the patient receives a kidney transplant while high antibody titers persist, recurrence may develop in the transplant. In a small subset of patients with Alport syndrome, a genetic disease due to mutation of a type IV collagen chain, the normal type IV collagen in the transplant may be recognized as foreign, and similar anti-GBM antibody disease may occur.
Linear accentuation by IgG of the GBMs may be present in diabetic injury, but there are no crescents or necrosis in diabetic nephropathy, which is characterized by nodular sclerosis. Linear GBM staining is present in monoclonal immunoglobulin deposition disease, the most common form of which is light chain deposition disease. This shows mesangial expansion, typically nodular, along with tubular basement membrane staining with monoclonal light chain, with powdery corresponding deposits by EM.
Crescentic lesions may be seen in various immune complex diseases, diagnosed by disease-specific IF and EM findings, typically with endocapillary hypercellularity. Pauci-immune necrotizing crescentic glomerulonephritis has little or no staining by IF, with none or few deposits by EM. Crescents typically vary more by stage of activity and chronicity than seen in anti-GBM antibody–mediated glomerulonephritis.
Definitive distinction requires IF.