Microscopy Images
Pauci-immune necrotizing crescentic glomerulonephritis is the pattern of injury most commonly seen with ANCA-associated glomerulonephritis.
This may present as granulomatosis with polyangiitis (GPA, formerly known as Wegener granulomatosis), microscopic polyangiitis (MPA), eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg-Strauss syndrome), or be renal limited. More than 85% of patients with active disease have positive ANCA.
The kidney manifestations are indistinguishable in these entities, and most patients present with systemic vasculitis and rapidly progressive glomerulonephritis.
Further distinctions are made based on the extrarenal patterns of involvement. GPA patients more often have pulmonary and ear, nose, and throat involvement, and proteinase 3 (PR3)-ANCA. MPA patients more often have myeloperoxidase (MPO)-ANCA, but both have frequent kidney disease. EGPA is considered when the patient also has asthma with eosinophilia; only about half of patients have kidney disease. These vasculitides can occur at any age, but patients most often are middle-aged, with equal incidence by sex. Fever, purpuric skin lesions, and arthralgias and myalgias are common. If left untreated, there is high (~80%) mortality at 1 year; with aggressive treatment, patient and kidney survival at 5 years is 75%. The disease course is typically relapsing and remitting, with longterm prognosis apparently slightly better in those with MPO-ANCA than those with PR3-ANCA. A higher proportion (>50%) of histologically normal glomeruli at biopsy is an excellent predictor of better kidney function at follow-up.
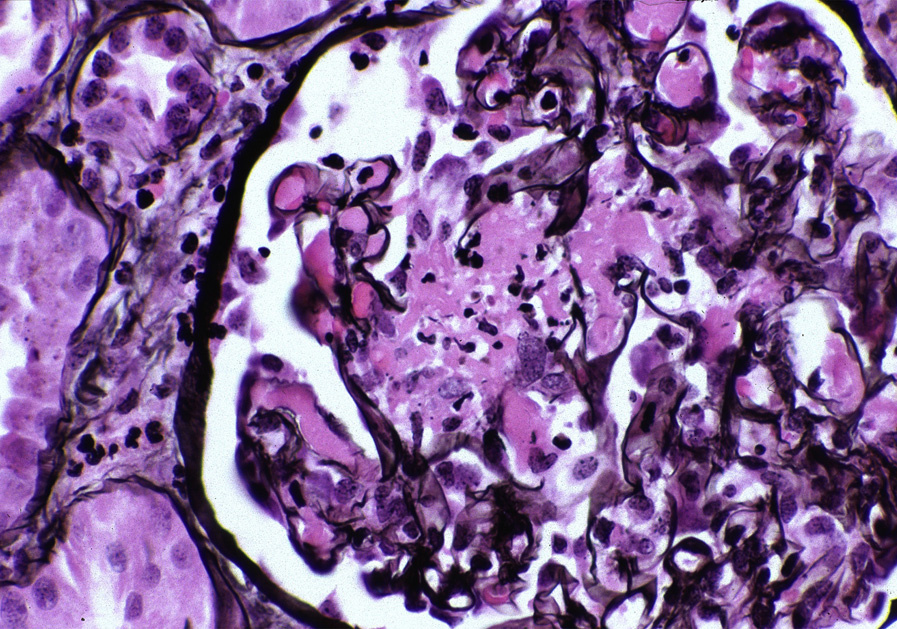
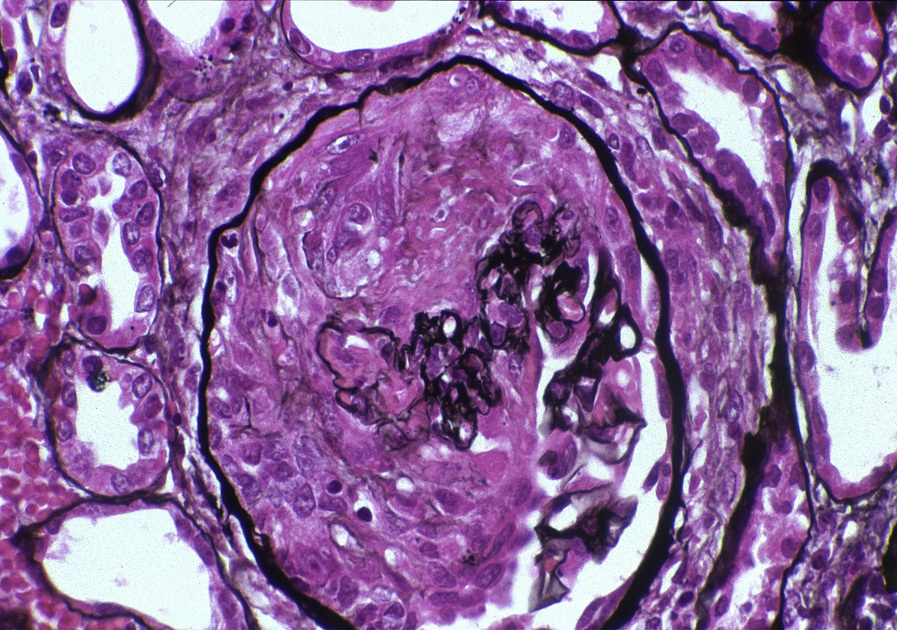
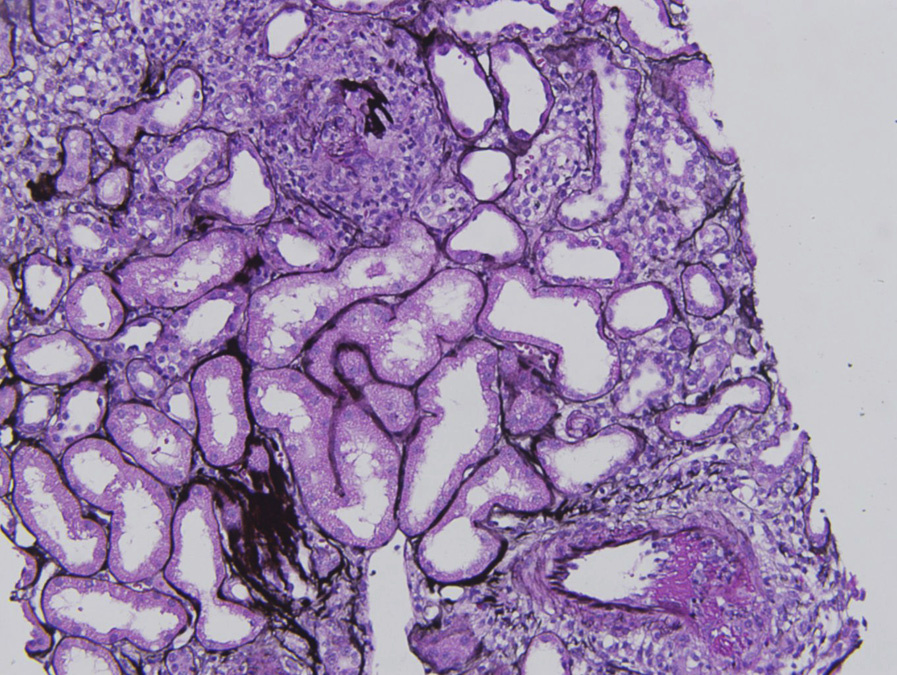
Light microscopy: Glomeruli show segmental glomerular basement membrane (GBM) breaks, necrosis, and crescents, often at varying stages of organization, ranging from cellular to fibrocellular to fibrous. Unaffected portions of the glomeruli do not show significant proliferation.
Periglomerular inflammation, even granulomatous, is associated with Bowman capsule breaks. Granulomatous inflammation, particularly in the small airways, is characteristic of GPA and EGPA, but not MPA. Interstitial granulomas are not typically seen in kidney biopsies in any of these entities. Small arteries also can show fibrinoid necrosis involving arterioles and interlobular arteries, often with surrounding perivascular inflammation that may also have a granulomatous appearance. There is proportional tubular injury with RBC casts, and in chronic cases, tubular atrophy with interstitial fibrosis.
Immunofluorescence microscopy: There is limited, if any, staining for immunoglobulins by IF.
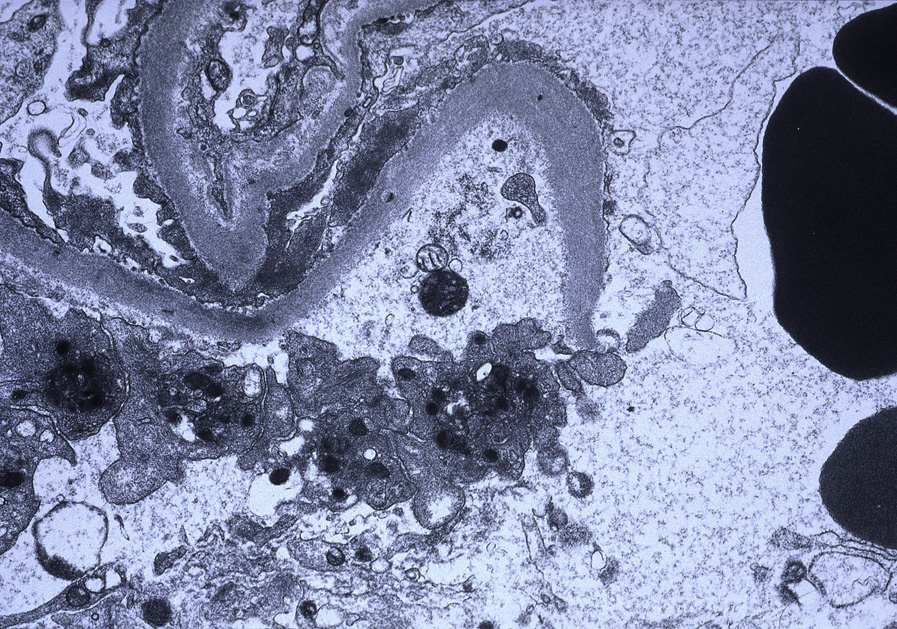
Electron microscopy: There are few, if any, immune complex–type deposits. GBM breaks, fibrin tactoids, and crescents are present.
ANCA are now shown to play a key role in pauciimmune necrotizing crescentic glomerulonephritis, not just as a marker of disease but also in the pathogenesis.
ANCA react with neutrophils, activating them to release injurious factors that activate alternative complement.
This feeds into a vicious cycle of more neutrophil attraction and more neutrophil activation. Activated neutrophil adherence to endothelial cells causes direct cellular injury and necrosis. Synergistic events such as upper respiratory tract infections can initiate this cascade by priming neutrophils, which then are activated by ANCA. The initiating events for formation of ANCA autoantibodies are unproven, but immune responses to an infectious agent have been postulated.
Anti-GBM antibody–mediated glomerulonephritis is distinguished by linear anti-GBM staining with IgG by IF. Of note, this entity cannot be distinguished from pauci-immune necrotizing crescentic glomerulonephritis by EM, since neither shows deposits. Subacute bacterial endocarditis–associated glomerulonephritis may have limited deposits; hump-type subepithelial deposits, dominant C3, and IgM by IF favor this entity over pauci-immune necrotizing crescentic glomerulonephritis. GPA, MPA, and EGPA or renal-limited pauci-immune necrotizing crescentic glomerulonephritis cannot be distinguished by kidney biopsy.