Microscopy Images
Antibiotic therapy has decreased the incidence of glomerulonephritis related to subacute bacterial endocarditis (SBE). Kidney involvement may be the initial manifestation of SBE in about 20% of patients.
Hematuria and mild proteinuria are commonly present. Hypertension and nephrotic syndrome are rare.
Serum complement levels may be low. Gross hematuria may be present in patients with renal infarctions related to embolic events. The degree of GFR loss correlates with the severity of glomerulonephritis; diffuse glomerulonephritis causes moderate GFR loss, and necrotizing glomerulonephritis with crescents can cause a rapid GFR decline. More extensive glomerulonephritis is commonly associated with high-titer ANCA positivity. Antibiotic therapy can result in partial to complete resolution of kidney disease.
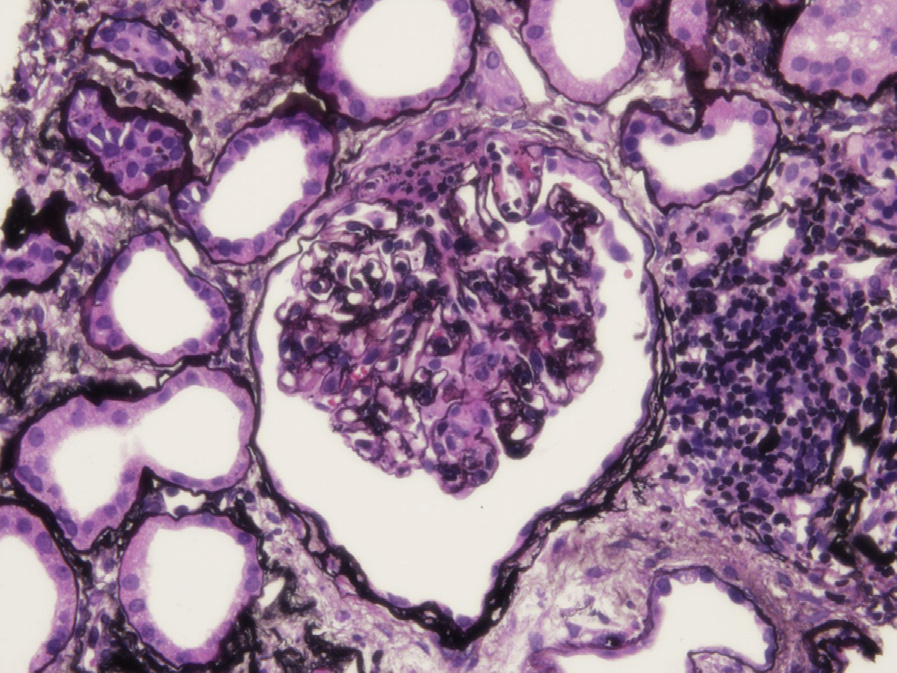
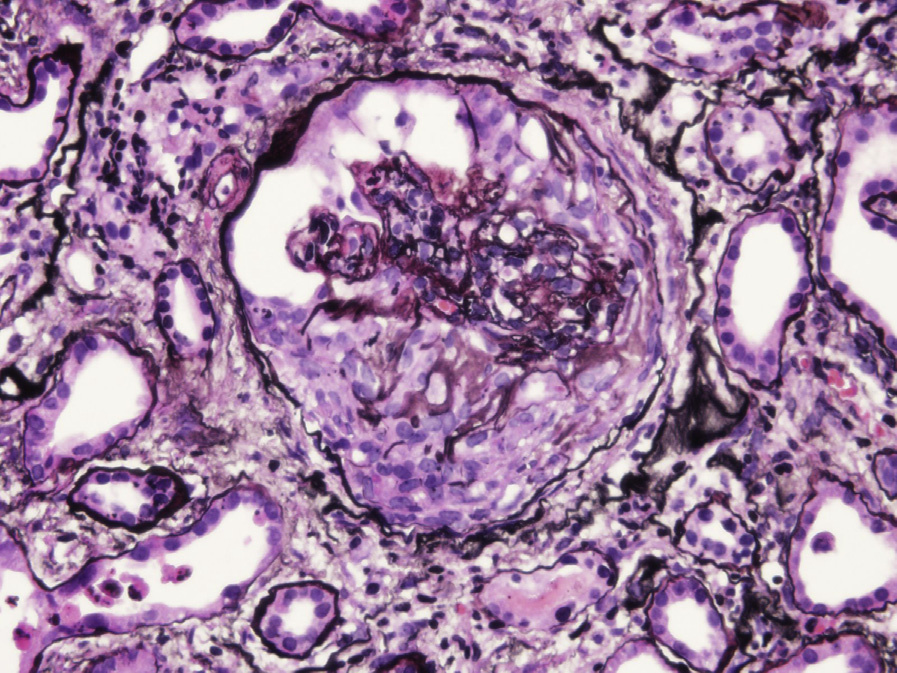
Light microscopy: Glomerular lesions show variable and often mixed active and chronic lesions. Focal or diffuse proliferative glomerulonephritis is present in about half of cases, and may have neutrophils within the glomerular tuft. Focal necrotizing lesions with crescents may be present. Chronic lesions include segmental glomerulosclerosis, as well as fibrocellular and fibrous crescents. Renal infarction related to an embolic event can occur. Necrotizing glomerulonephritis with crescents without endocapillary hypercellularity can occur.
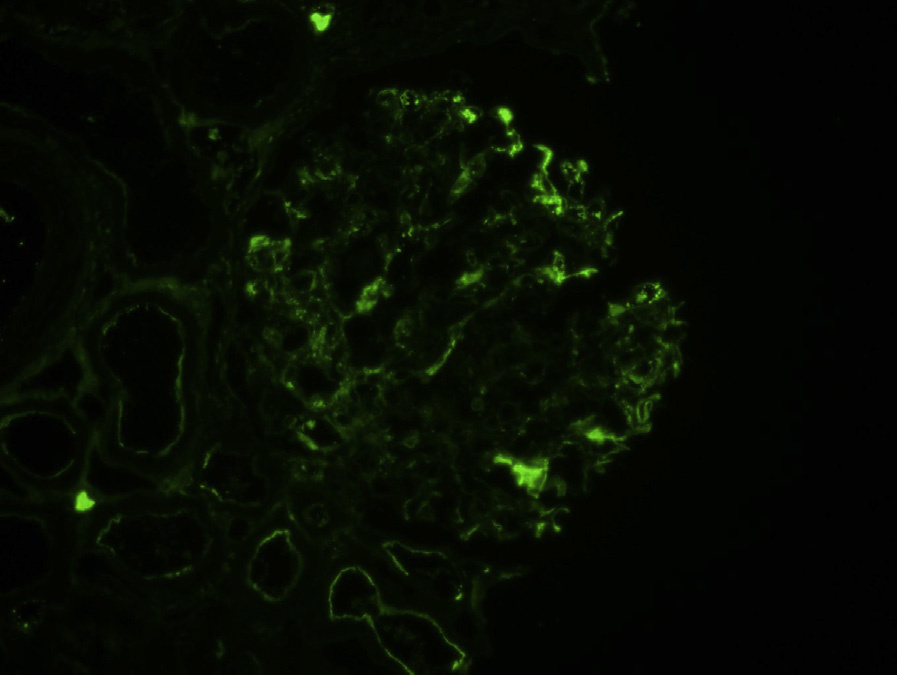
Immunofluorescence microscopy: Mesangial and capillary wall irregular, granular staining for IgG, IgM, C3, and sometimes IgA are usually present in cases with proliferative glomerulonephritis.
IgM staining is usually greater than IgG and IgA. IgA may be dominant in cases with staphylococcal infection.
However, there is typically little or no staining in cases with necrotizing glomerulonephritis with crescents.
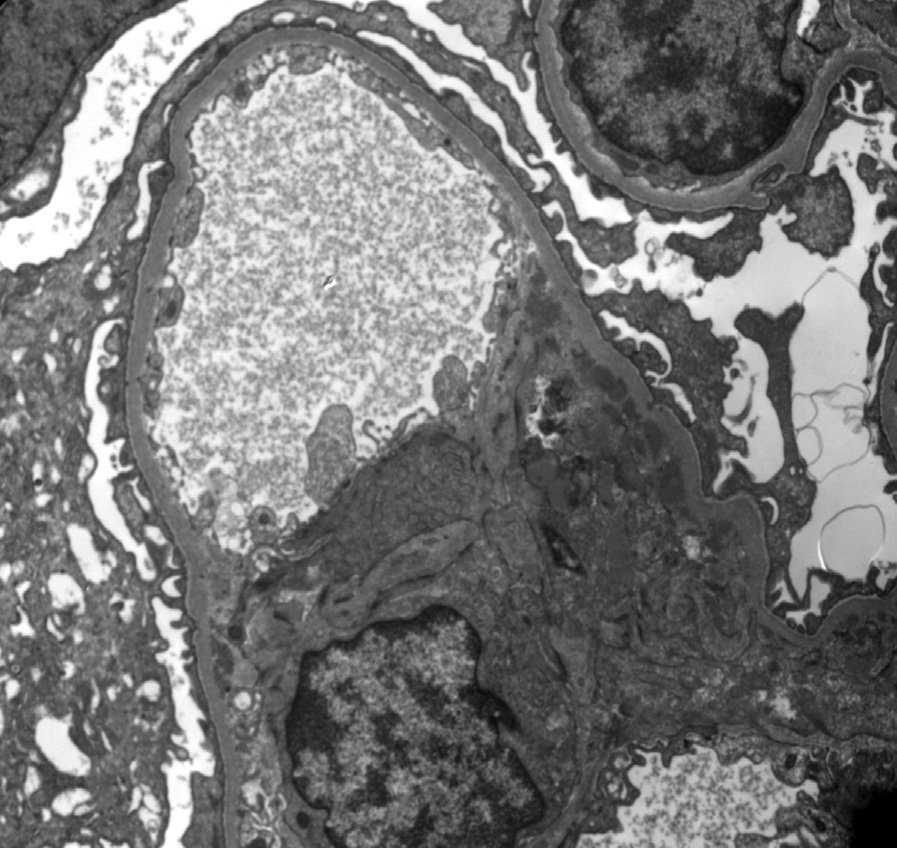
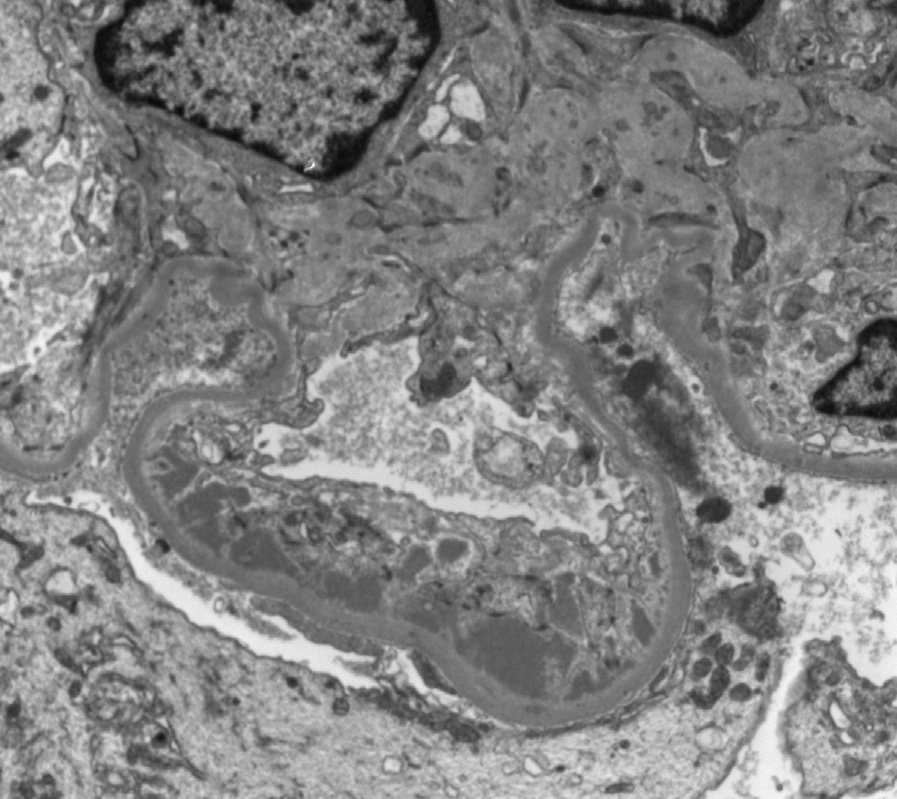
Electron microscopy: Subepithelial, subendothelial, and mesangial deposits may be seen. The extent of subendothelial deposits correlates with the extent of proliferation present by light microscopy.
Subepithelial hump-type deposits may be present. Cases with necrotizing glomerulonephritis without proliferation may have few or no deposits.
Circulating immune complexes related to infectious endocarditis cause proliferative lesions, supported by the presence of immunoglobulin and complement staining by immunofluorescence, and deposits by electron microscopy. In cases with little or no immune complex deposition, ANCA may have a pathogenic role.
SBE with focal necrotizing crescentic lesions with little or no staining by immunofluorescence microscopy, and few if any immune complex deposits by electron microscopy, may be indistinguishable morphologically from ANCA-associated pauciimmune necrotizing crescentic glomerulonephritis.
However, SBE-associated necrotizing glomerulonephritis is typically less extensive than that caused by ANCA. Infections in other sites than SBE can cause similar findings. Clinical correlation is needed to determine source of infection. Lupus nephritis can have focal or diffuse proliferation with necrotizing lesions. A “full-house” pattern of immunofluorescence staining with tubuloreticular aggregates and clinical history of lupus with corresponding serology helps distinguish a lupus etiology.