Microscopy Images
Chronic kidney disease (CKD) associated with hypertension disproportionately affects African Americans, and occurs at younger age (as young as 20s) and with faster progression than in whites. Men are affected more than women. Patients develop progressive proteinuria that is related to the severity of hypertension, and may even have nephrotic range proteinuria. Hypertension-associated CKD accounts for approximately 25% of patients reaching end-stage kidney disease. Intensive therapy with antihypertensive drugs, including renin-angiotensin blockade, slows progression. Malignant hypertension can present with additional findings including congestive heart failure, acute kidney injury, and microangiopathic hemolytic anemia.
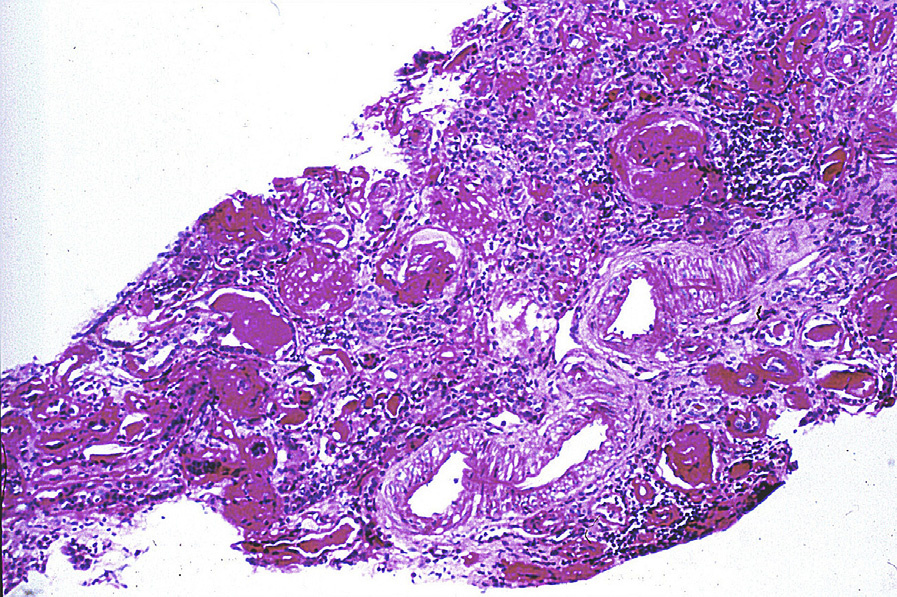
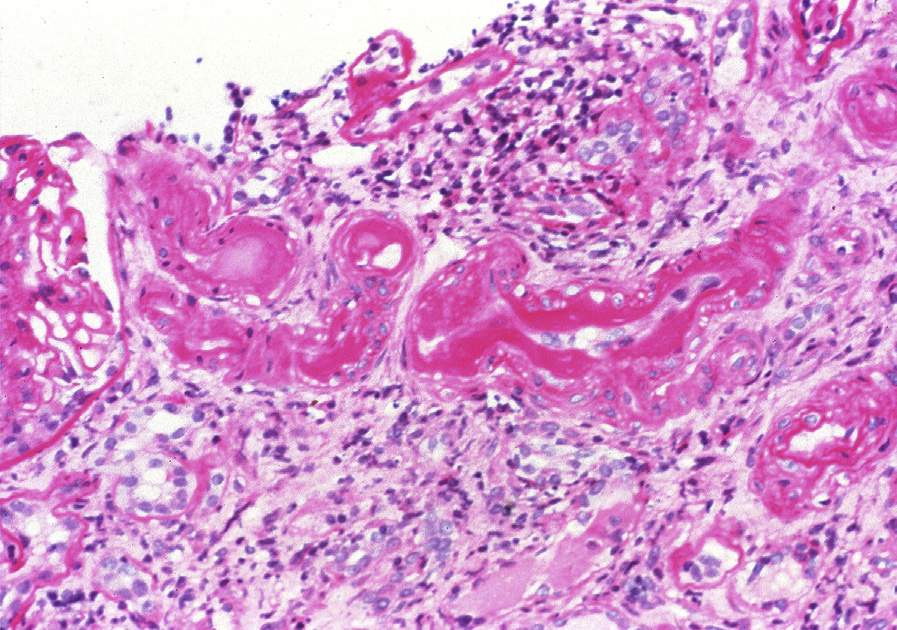
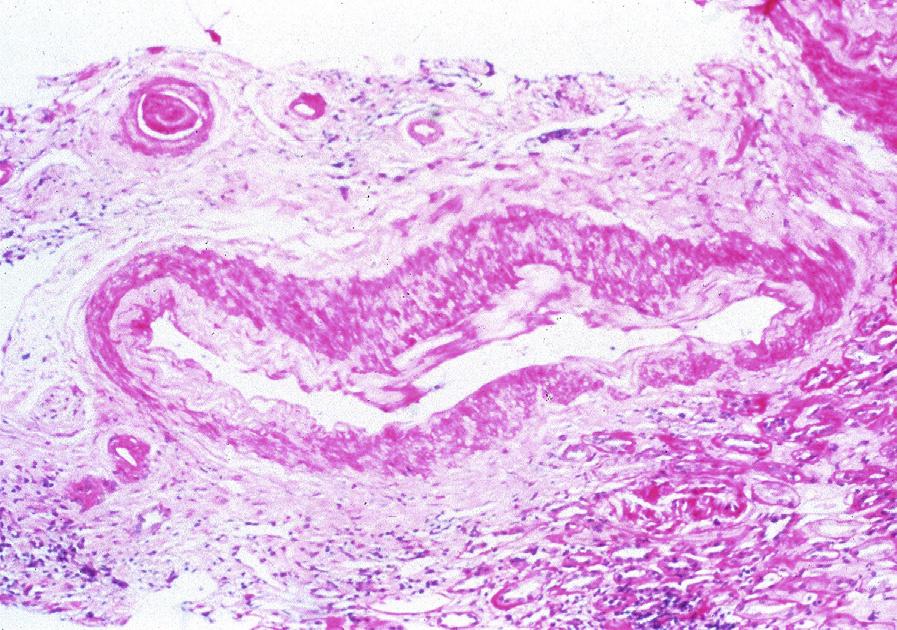
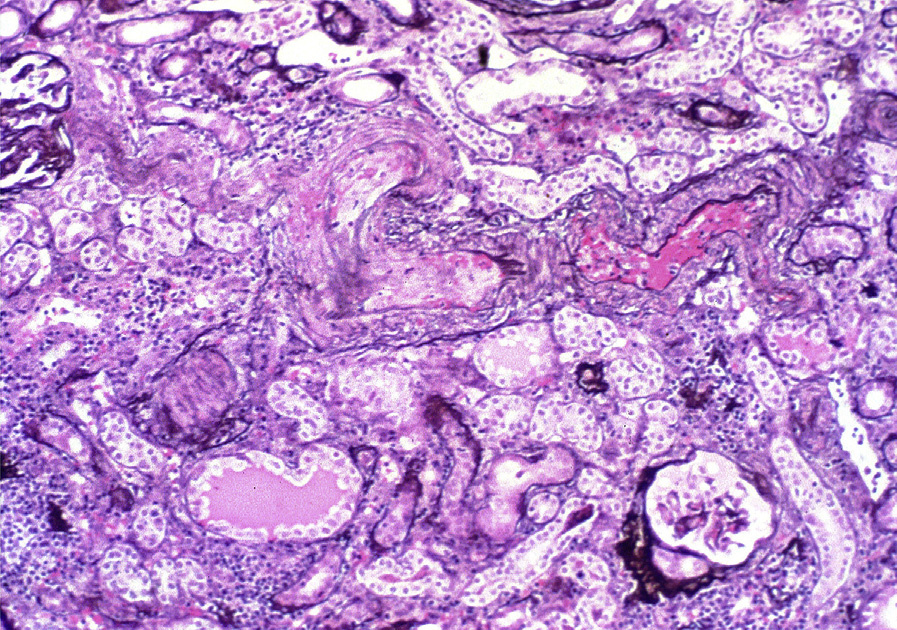
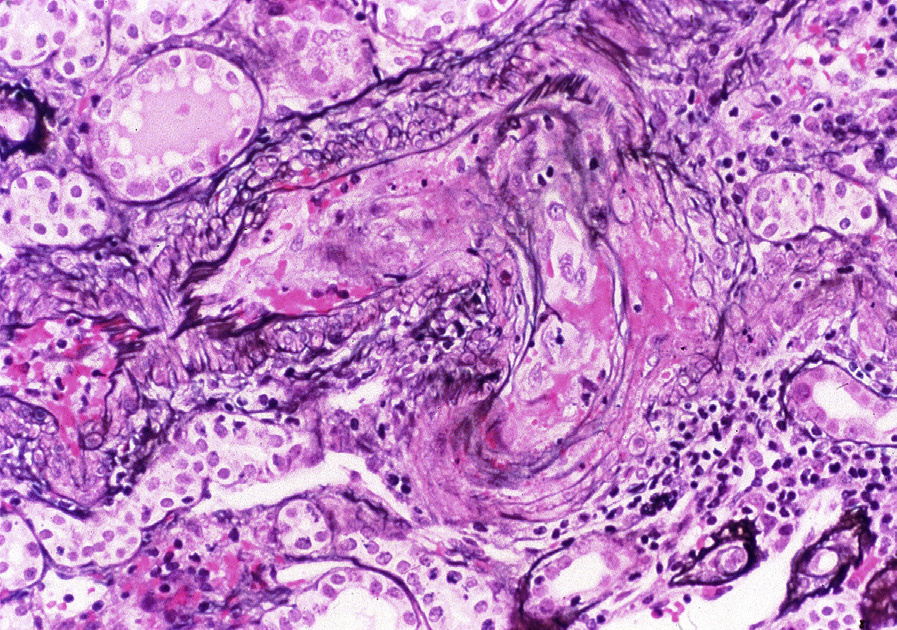
Light microscopy: Hypertension-associated kidney disease is characterized by arterionephrosclerosis, with medial thickening, intimal fibrosis, and tortuosity of medium- and large-sized arteries. There is medial thickening and hyalinosis of arterioles, frequently associated with global glomerulosclerosis and often seen in a solidified pattern. Secondary segmental sclerosis can occur, particularly in a perihilar location. There is proportional tubulointerstitial fibrosis.
With accelerated hypertension-associated injury, there is mucoid change of the arteries. Endothelial swelling and red blood cell fragments may be present in the arterial wall, and medial hypertrophy of small interlobular arteries in a concentric pattern with luminal stricture, the so called “onion skinning,” may be seen. In malignant hypertension, fibrinoid necrosis of the wall of arterioles and/or interlobular arteries often occurs with red blood cell fragments and fibrin within the lumen. Glomerular involvement with fibrin thrombi is uncommon.
Immunofluorescence microscopy: Immunoglobulin M, C3, and C1q staining may be seen in areas of hyalinosis. Fibrinogen staining will occur in areas of fibrinoid necrosis or when thrombotic microangiopathy is present in malignant hypertension.
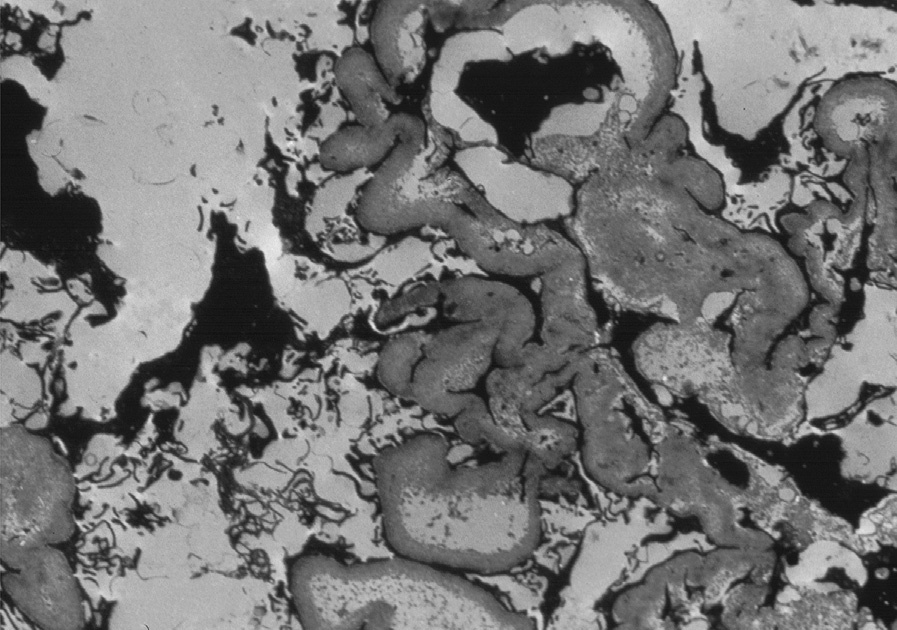
Electron microscopy (EM): Glomerular basement membranes may be moderately thickened and corrugated. There is expansion of lamina rara interna and segmental cellular interposition related to chronic endothelial injury. Foot process effacement is variable, but may be extensive, particularly in areas of secondary segmental sclerosis.
In malignant hypertension–associated injury, fibrin tactoids may also be present. Vascular changes parallel those seen by light microscopy.
Hypertension-attributable CKD is markedly increased in African Americans, and particularly associated with the G1 and G2 risk allele variants of apolipoprotein AI, compared to G0. These allele variants are protective against some forms of trypanosomal disease, which may, due to evolutionary pressures, explain increased incidence in those of African ancestry. The mechanisms for the marked increased risk of hypertension-associated CKD are unknown.
Primary focal segmental glomerulosclerosis can have both segmental and global glomerulosclerosis; however, the background vascular changes are more extensive in arterionephrosclerosis and may show more limited foot process effacement by EM. Diabetic nephropathy also has hyalinosis of arterioles but characteristically involves both afferent and efferent arterioles with nodular mesangial expansion and diffuse thickening of glomerular basement membrane shown by EM. Systemic sclerosis has identical biopsy findings as those in malignant hypertension–associated kidney disease, requiring clinical history to distinguish these etiologies.