Microscopy Images
Systemic sclerosis (scleroderma) has a strong predilection in women, with onset typically between ages 30-50 years. Scleroderma kidney disease occurs in 60%-70% of patients with systemic scleroderma, mostly in those with a diffuse, rather than limited, form of cutaneous scleroderma. Kidney disease is evident by hypertension, proteinuria, and loss of glomerular filtration rate. Scleroderma kidney crisis develops in about 10%-20%, and presents as new onset malignant hypertension with acute kidney injury. Antinuclear antibody is positive in >90% of these patients. Anti-topoisomerase 1 and anti-RNA polymerase antibodies are often associated with kidney involvement. Patients with scleroderma kidney crisis may require dialysis.
Use of angiotensin-converting enzyme inhibitors has improved prognosis of patients with kidney crisis, but mortality at 5 years remained at 30%-40%.
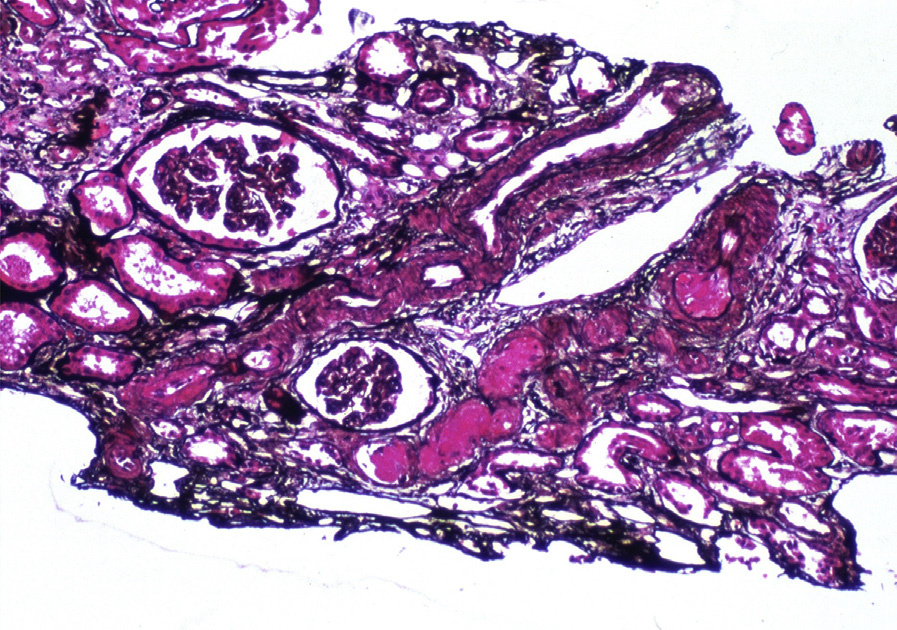
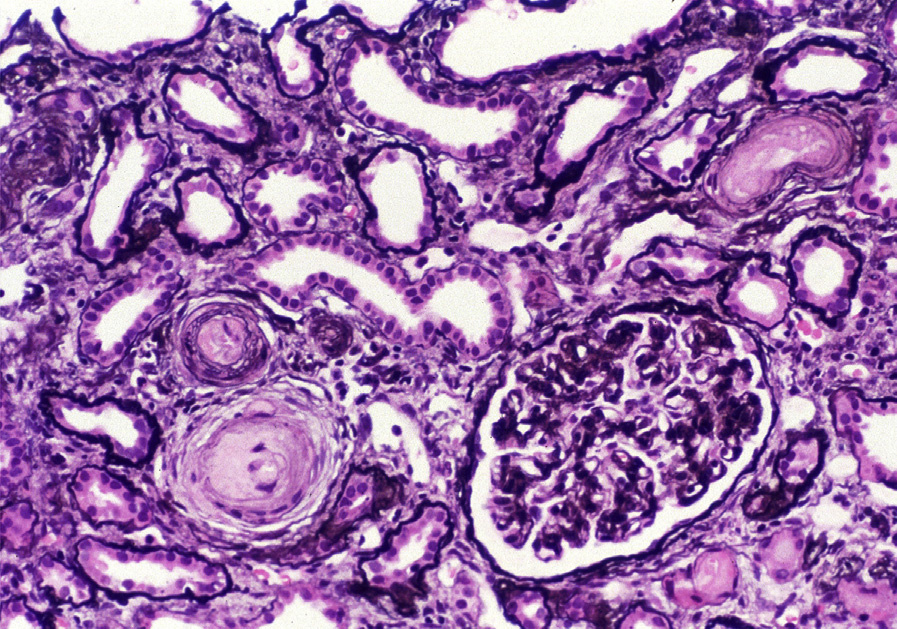
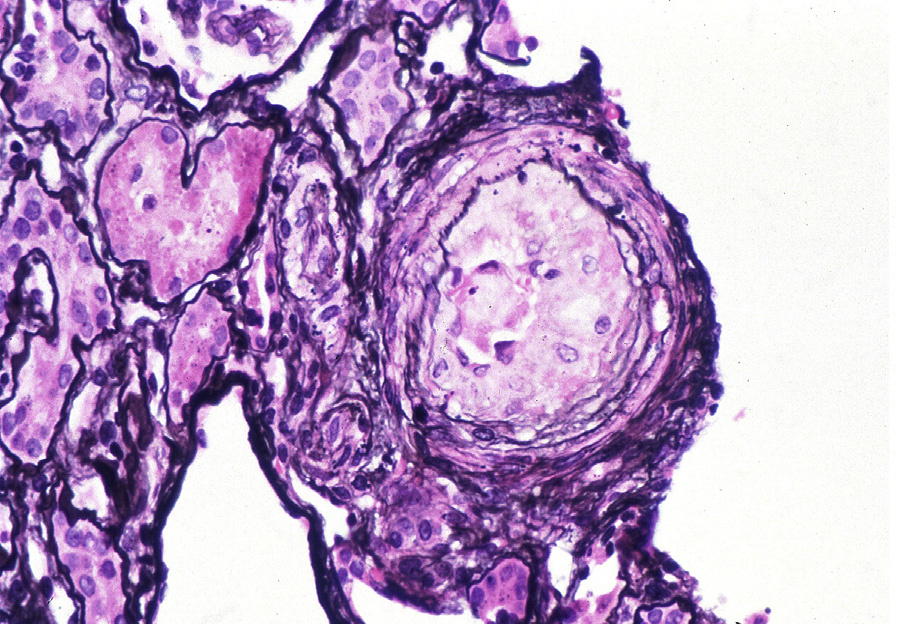
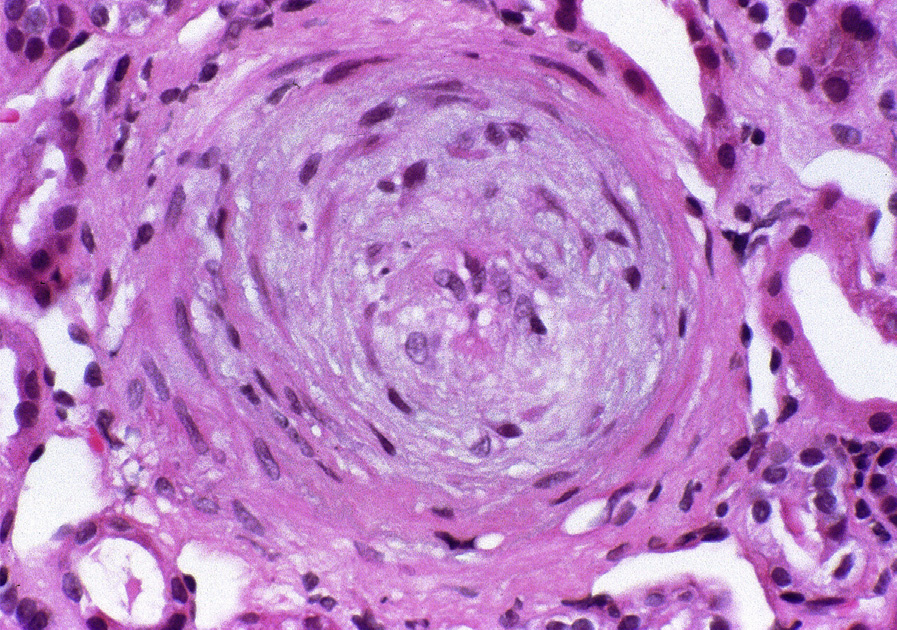
Light microscopy: Medium- and large-sized arteries are affected by thrombotic microangiopathy. Fibrin thrombi with fibrinoid necrosis of the vessel wall without associated wall inflammation are characteristic. Intimal mucoid change, endothelial swelling, and fragmented red blood cells within the vessel wall occur acutely. Later, there is intimal proliferation, resulting in an “onion skin” concentric appearance with luminal narrowing. Glomeruli typically show ischemic collapse, but may also have mesangiolysis and fibrin thrombi. Glomerular basement membrane duplication is present in chronic cases. Tubular injury occurs with acute injury, and tubular atrophy and interstitial fibrosis are proportional to vascular injury in the chronic stages.
Immunofluorescence microscopy: Nonspecific staining for immunoglobulin M and C3 may be seen.
Fibrinogen staining can be observed in glomeruli and arteries associated with fibrinoid necrosis or acute thrombotic microangiopathy.
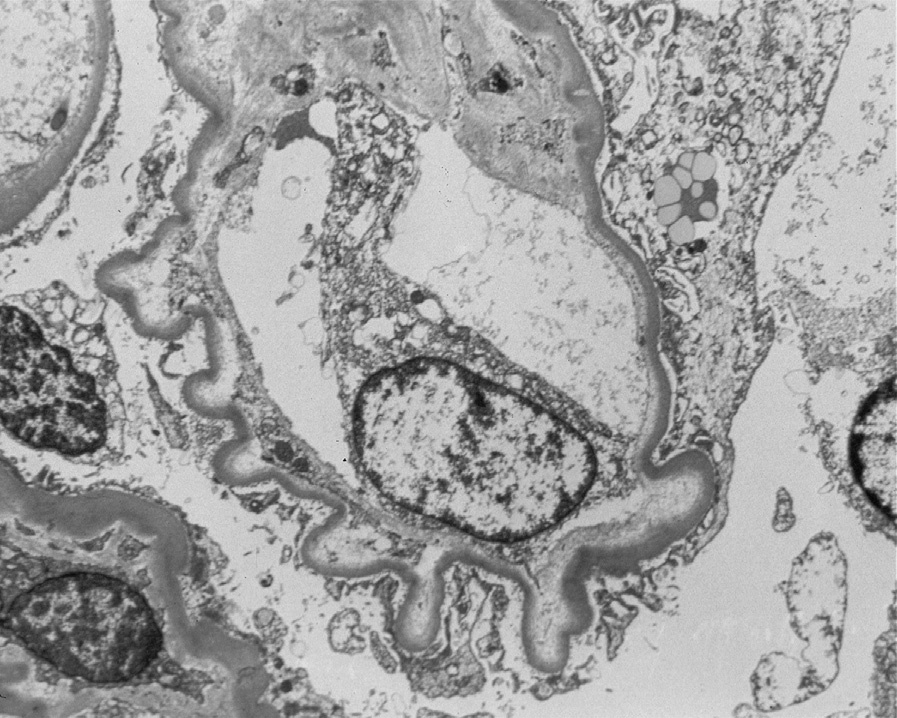
Electron microscopy: Endothelial swelling and expansion of lamina rara interna are present. Glomerular basement membrane duplication with cellular interposition is present in chronic stages.
Injury from scleroderma is related to endothelial injury of uncertain etiology. About half of patients have anti-endothelial antibodies. Endothelial injury leads to altered vascular permeability and platelet aggregation.
Increased renin production exacerbates hypertension.
Thrombotic microangiopathy of other causes has similar morphologic findings, including malignant hypertension, drug etiology, complement dysregulation, hemolytic uremic syndrome/thrombotic thrombocytopenic purpura (HUS/TTP), and transplant rejection.
Scleroderma mostly affects interlobular arteries in contrast to HUS/TTP, which predominantly affects glomeruli. Malignant hypertension-associated thrombotic microangiopathy may have an identical appearance to that seen in scleroderma, although this is more often associated with underlying arterionephrosclerosis. Clinical history and serologic data help to distinguish these etiologies.