Microscopy Images
Cholesterol emboli usually occur in patients older than 50 years with a predilection in men and whites.
Clinical presentation includes acute kidney injury, new onset hypertension, proteinuria that may be in the nephrotic range, hematuria, and occasionally increased eosinophils. Cholesterol emboli can involve all organs downstream of atherosclerotic plaques, including the lower extremities where it manifests as livedo reticularis. The kidney is the most common site of involvement, followed by the spleen, pancreas, gastrointestinal tract, and adrenal glands. Prognosis overallis poor, related to theunderlying severe vascular disease and multi-organ complications.
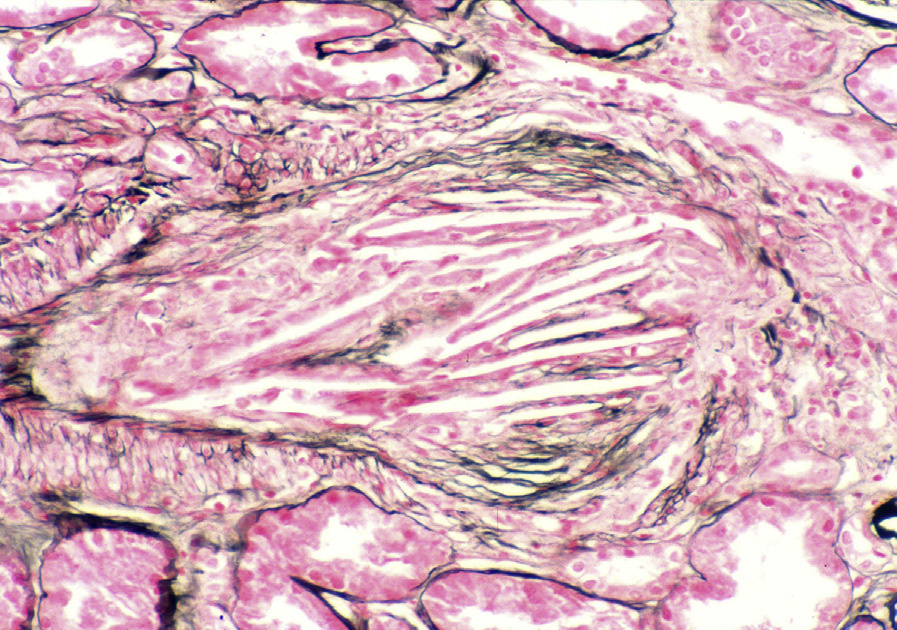
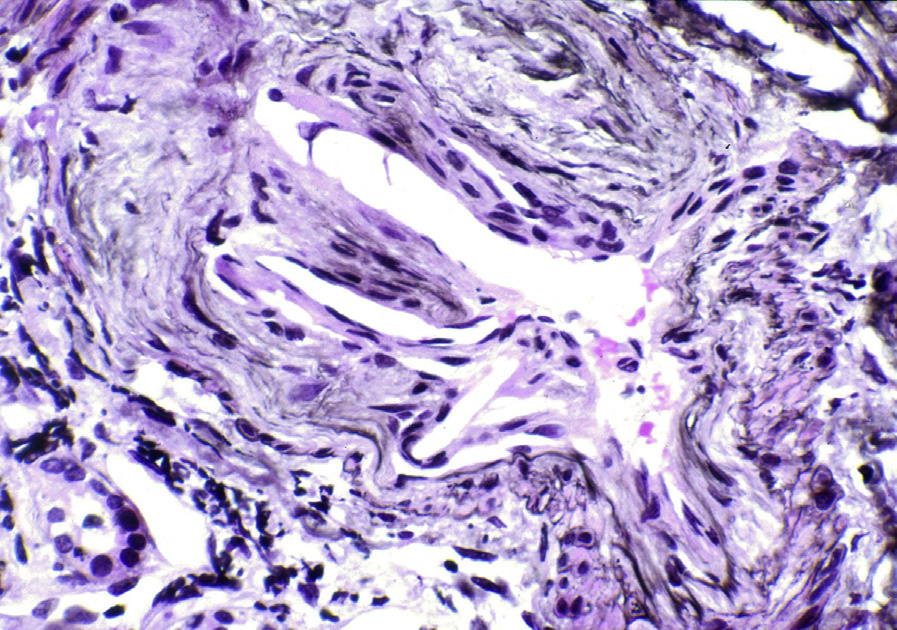
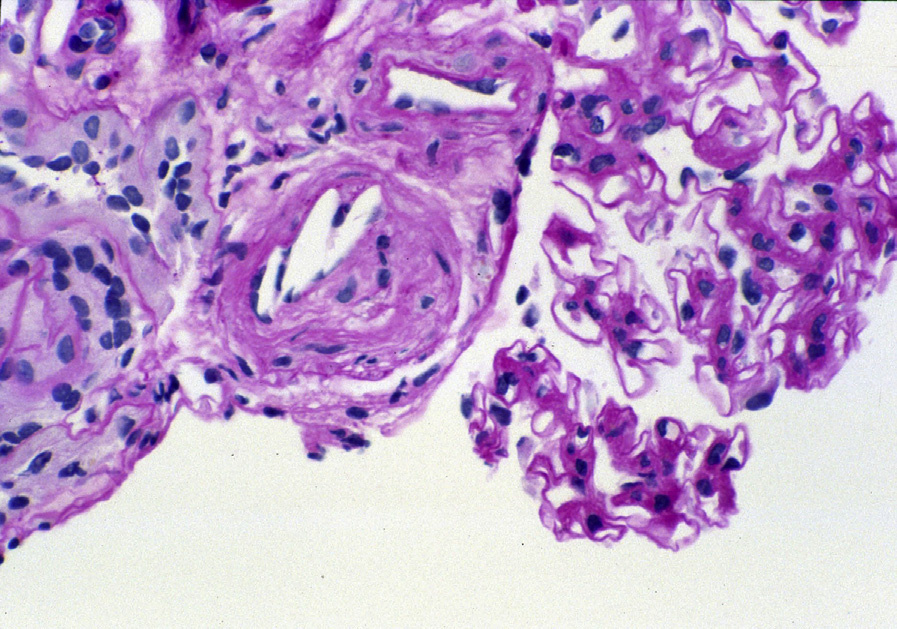
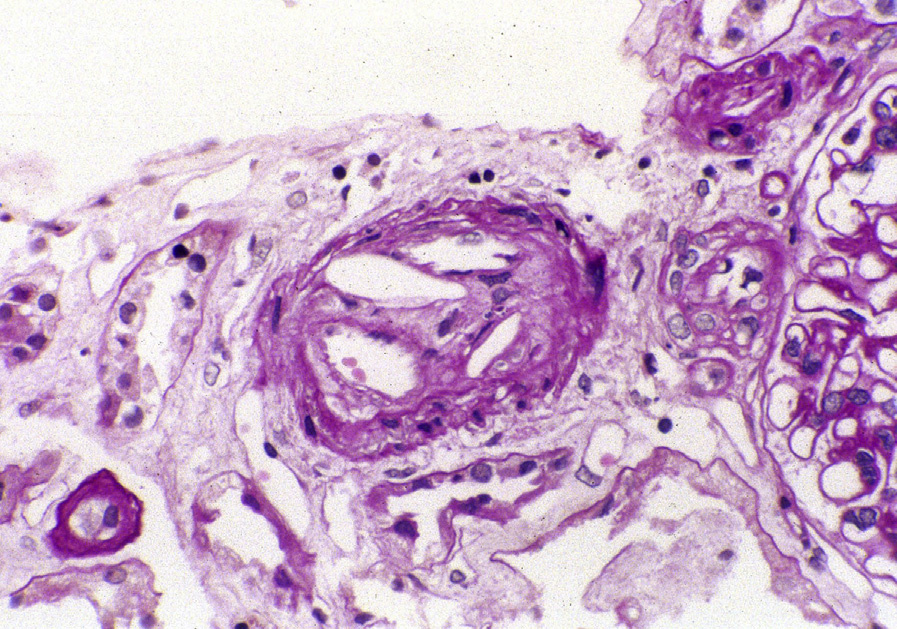
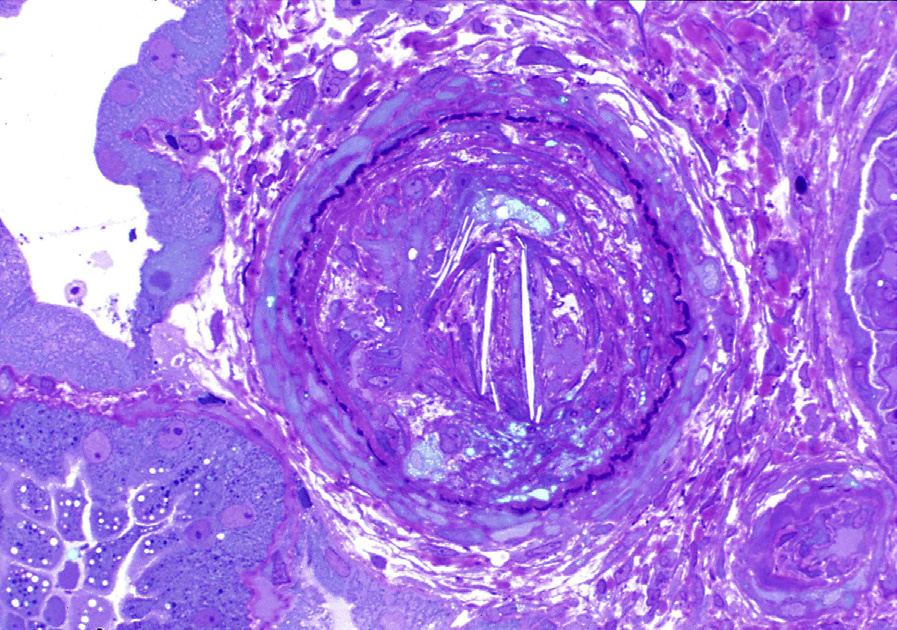
Light microscopy: Atheroemboli are visualized as lance-shaped clefts, due to dissolution of cholesterol crystals during formalin fixation. They occur most commonly in interlobular and arcuate arteries, but may also involve arterioles and rarely reach glomeruli.
Acute lesions are often surrounded by red blood cells, fibrin, and leukocytes, with multinucleated giant cell reactions in the subacute phase. Chronic lesions show intimal fibrosis surrounding the cholesterol clefts.
Vessel recanalization of chronic lesions can occur.
Global and segmental sclerosis of glomeruli may be present. In cases of massive cholesterol emboli, zonal areas of tubular necrosis may occur.
Immunofluorescence microscopy: No specific staining is seen.
Electron microscopy: Extensive foot process effacement may be present.
Cholesterol emboli occur due to rupture and embolization of portions of atherosclerotic plaques.
Risk factors are those for atherosclerotic disease, with markedly increased risk after abdominal aortic instrumentation for procedures such as coronary artery angiography/angioplasty or vascular surgery such as aortic aneurysm repair. Cholesterol emboli may, however, even occur spontaneously without vascular procedures. Manipulation of anastomosing artery to the transplant during surgery could release cholesterol emboli into the newly transplanted kidney.
Renal artery stenosis can present with hypertension and show ischemic glomeruli with interstitial fibrosis and tubular atrophy. This may show a pattern of severe tubular atrophy that is out of proportion to interstitial fibrosis. Arterionephrosclerosis can have severe intimal fibrosis. The absence of cholesterol clefts distinguishes these entities from injury caused by cholesterol emboli.
Slit-like spaces due to vessel branching can be distinguished from cholesterol emboli by assessing serial sections.