Microscopy Images
Kidney disease is a common manifestation in HIV-infected patients. The spectrum of disease in HIV-infected patients varies, from HIV-associated nephropathy (HIVAN), which is manifest by collapsing glomerulopathy, to usual FSGS,minimal change disease, thrombotic microangiopathy, and lupus-like HIV-immune complex kidney disease (HIVICK). Other immune complex diseases may also occur in HIV-infected patients, including IgA nephropathy and postinfectious glomerulonephritis, and are best diagnosed as those specific entities. We thus restrict the diagnosis of HIVICK to the lupus-like lesions that are seen in some HIV-infected patients, without serologic evidence of lupus. HIVICK varies in frequency depending on the population studied. In HIV-infected patients of non-African ancestry with kidney biopsy, HIVICK appears to be more frequent than HIVAN. Patients with HIVICK have varying kidney manifestations, depending on the location and extent of glomerular deposits. A minority has concurrent HIVAN lesions. Proteinuria, which may be nephrotic, hematuria, reduced GFR, and low levels of complement are common. Patients may present at any age. Prognosis appears better than for HIVAN.
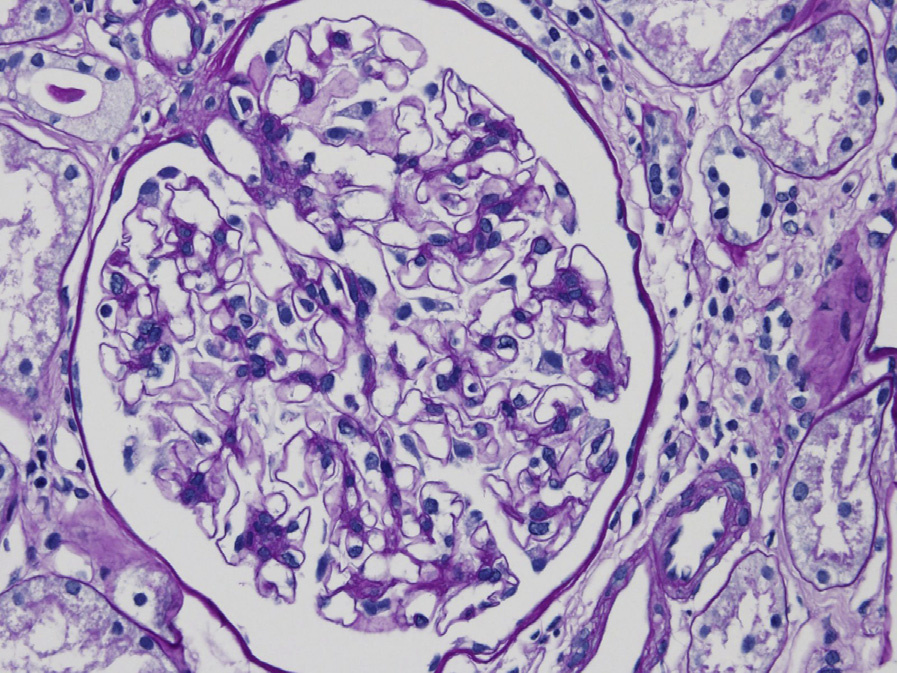
Light microscopy: Variable mesangial and focal or diffuse endocapillary hypercellularity are seen, with an occasional membranous pattern with corresponding pinpoint-hole appearance and spikes of the glomerular basement membrane on silver stain.
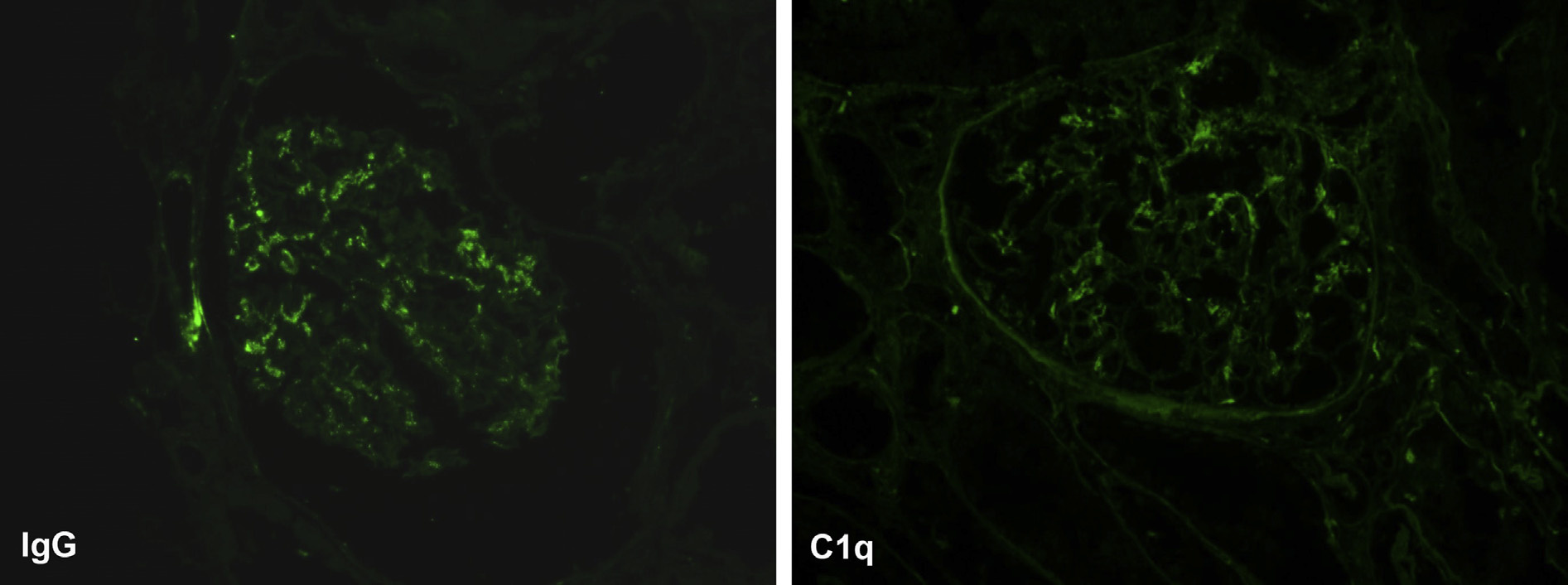
Immunofluorescence microscopy: “Full-house” staining with IgG, IgA, IgM, C3, and C1q granular staining in the mesangium and capillary loops.
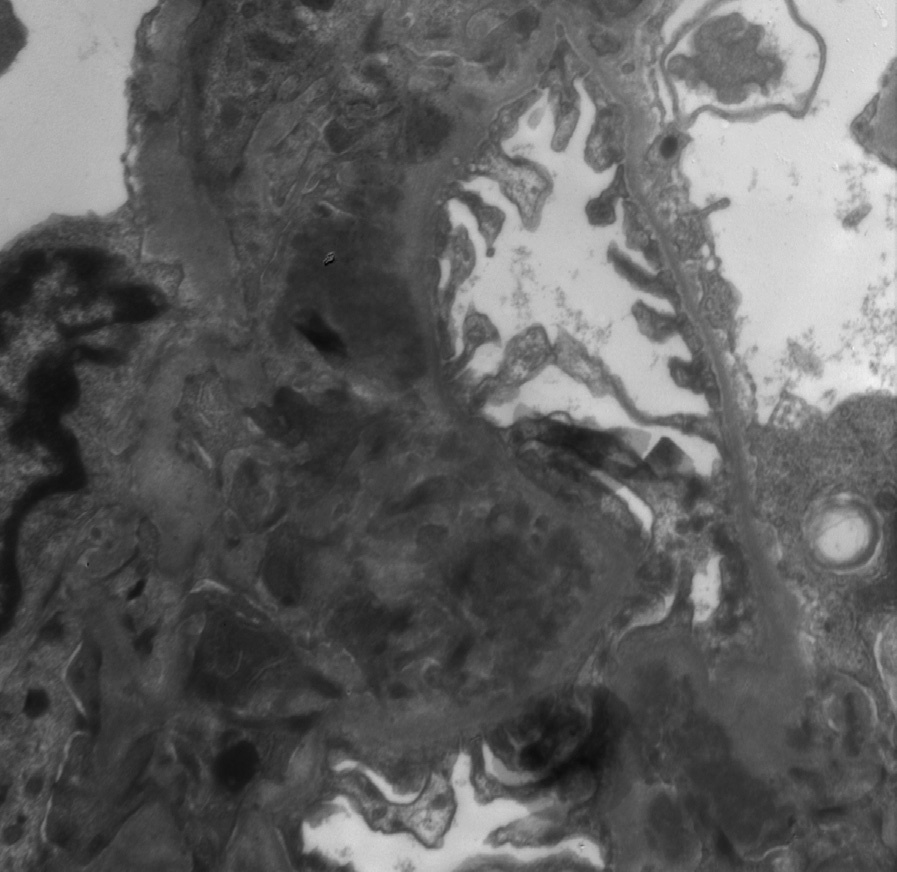
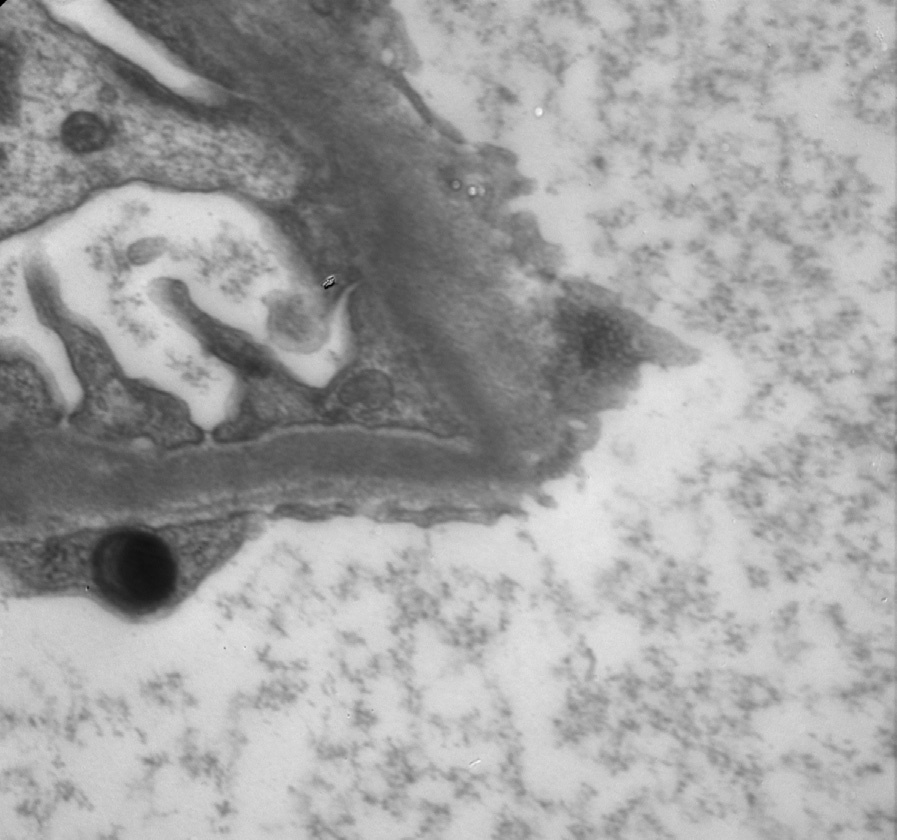
Electron microscopy: Variable deposits are seen, including mesangial, subendothelial, and subepithelial deposits, the latter extensive in cases with a membranous pattern. Tubuloreticular aggregates are present in endothelial cells. Tubuloreticular aggregates may be decreased or even absent in patients with low viral loads being treated with combination antiretroviral therapy.
HIVICK is due to HIV infection, with aberrant immune regulation and increased gamma globulin contributing to immune complex formation. This may involve HIV p24 (capsid) and gp120 (envelope) antigens as targets. APOL1 risk allele variants, common in African Americans, are not associated with increased frequency of HIVICK.
Lupus nephritis has similar morphologic features.
Distinction must be made on clinical grounds. The “ball-in-cup” appearance of some subepithelial deposits is not, in our opinion, specific for HIVICK, and may also be seen in lupus nephritis with membranous features.