Microscopy Images
The tip lesion variant of focal segmental glomerulosclerosis (FSGS) is associated with nephrotic syndrome and usually responds to steroid therapy.
This FSGS variant has the lowest risk for progression to kidney failure.
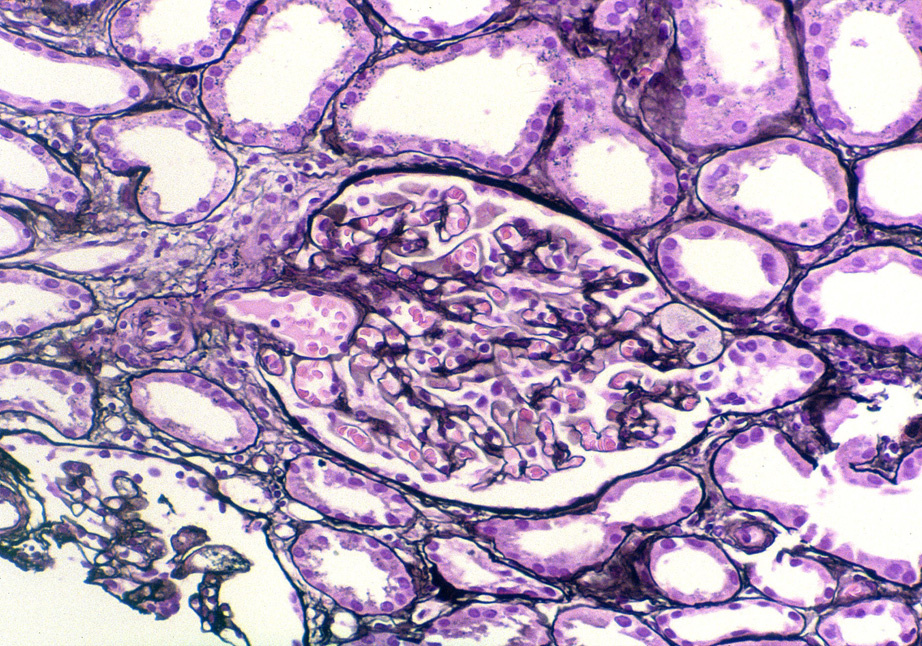
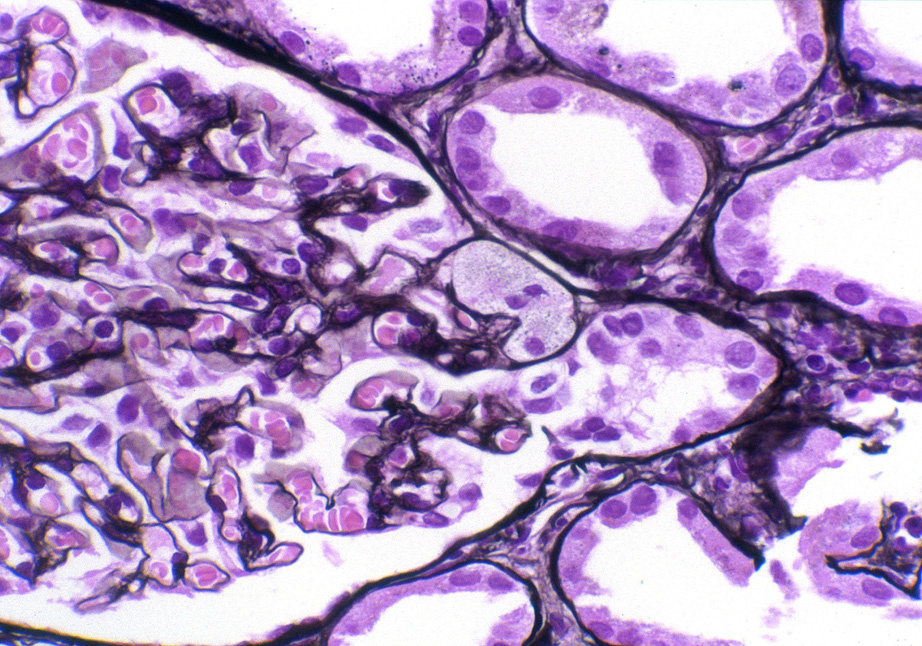
Light microscopy: Segmental glomerulosclerosis or endocapillary hypercellularity (usually foam cells) involving <50% of the glomerular tuft at the tubular pole, with an adhesion or confluence with tubular epithelium to the tubular outlet. Collapsing and perihilar variants must be excluded.
Immunofluorescence microscopy: No or limited deposits (nonspecific immunoglobulin M and C3 staining in sclerotic areas).
Electron microscopy: Extensive foot process effacement. No or limited deposits.
The etiology and pathogenesis of tip lesion has not yet been defined. Injury to podocytes by turbulent flow at the tubular pole has been proposed.
Usually of primary etiology, but may be seen in other diseases with heavy proteinuria (eg, membranous nephropathy).