Microscopy Images
Ischemic acute tubular injury describes a lesion of simplification of the tubules, which commonly manifests clinically as a rapid loss of glomerular filtration rate, often with oliguria, granular casts, and low-level proteinuria. Ischemic acute tubular injury may occur at any age, with varying underlying causality. Isolated acute tubular injury is often recoverable; however, the prognosis is poor if part of multiorgan failure. Episodes of ischemic acute tubular injury are now recognized to increase risk of chronic kidney disease long-term.
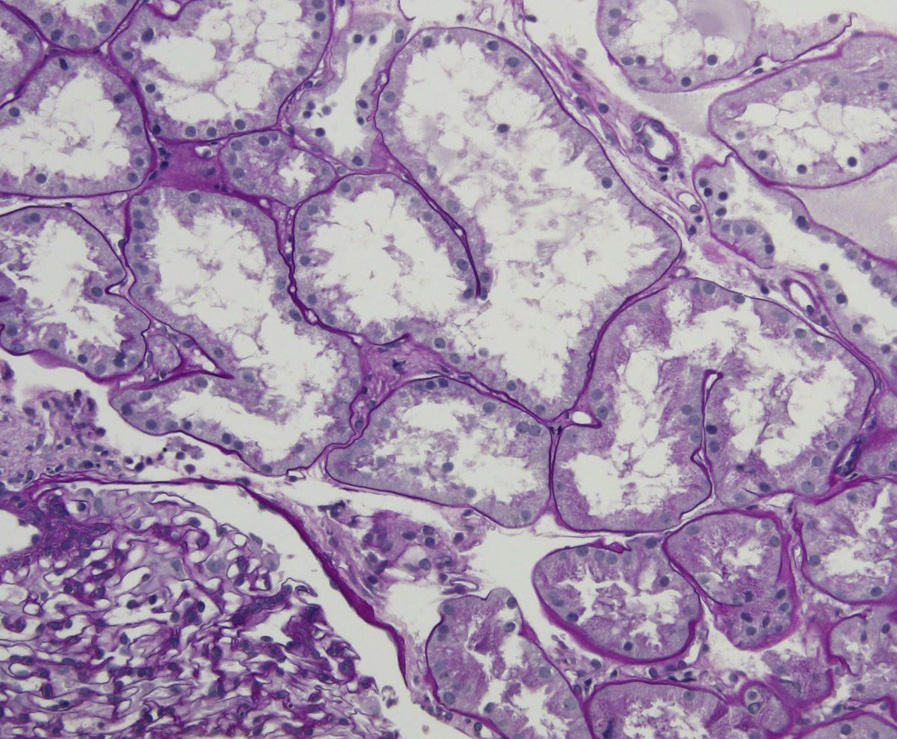
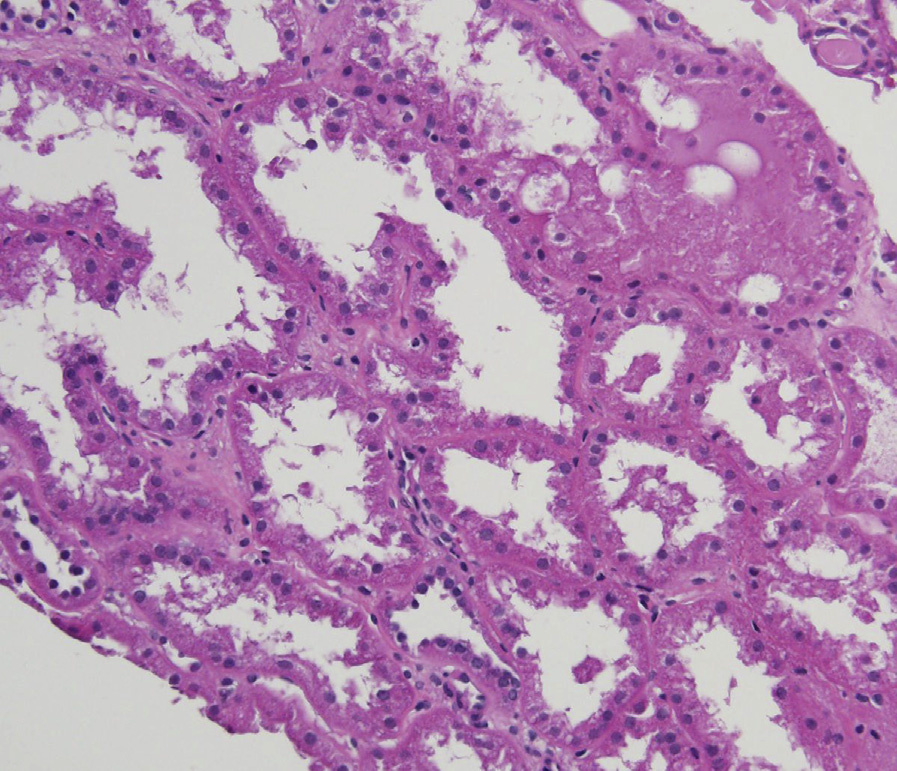
Light microscopy: The lesions predominantly affect the proximal tubules, with dilation of tubular lumens, flattening of epithelium, simplification and loss of brush border, and vacuolization. Granular casts may be present. The interstitium may show edema, but there is no significant inflammatory reaction in the acute phase, with mild interstitial inflammation as regeneration and repair ensue, with scattered lymphocytes, macrophages, and rare neutrophils and eosinophils.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: There is tubular injury with loss of brush border, and swollen injured mitochondria in tubular cells. Tubular cells may exhibit vacuolization, and simplification of interdigitating basolateral cell borders.
Hypotension or decreased perfusion due to hypovolemia or volume shifts are common underlying causes of ischemic acute tubular injury.
Dilated tubules may be seen in obstruction, but brush borders are intact. Dilated lumens are present in atrophic tubules, but the tubular basement membranes are thickened and there is increased interstitial matrix between tubules. Acute tubulointerstitial nephritis may have some tubular injury, but has a marked interstitial inflammatory component, with tubulitis.