Microscopy Images
Cortical necrosis commonly manifests clinically as a rapid loss of glomerular filtration rate, often with oliguria, granular casts, and low-level proteinuria. Cortical necrosis may occur at any age. Causes include complications of vascular anastomosis in the transplanted kidney. In the native kidney, it occurs after thrombosis of interlobular or larger arteries, massive cholesterol emboli, septic abortion, or other catastrophic obstetrical complications (including eclampsia), and in the neonate, it occurs as complications of sepsis and placental hemorrhage. Causes of native kidney cortical necrosis typically affect both kidneys. Prognosis depends on the underlying cause.
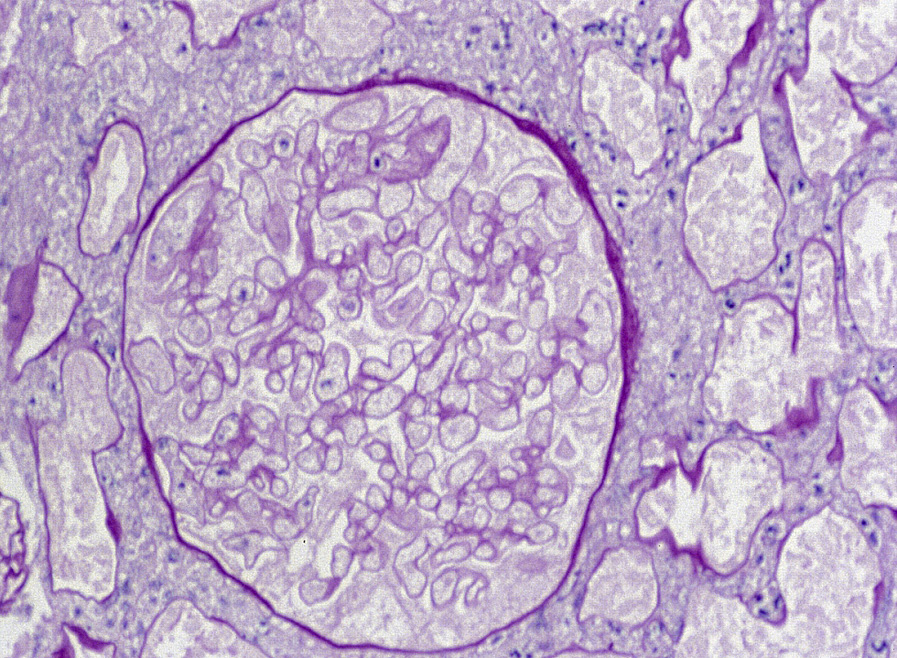
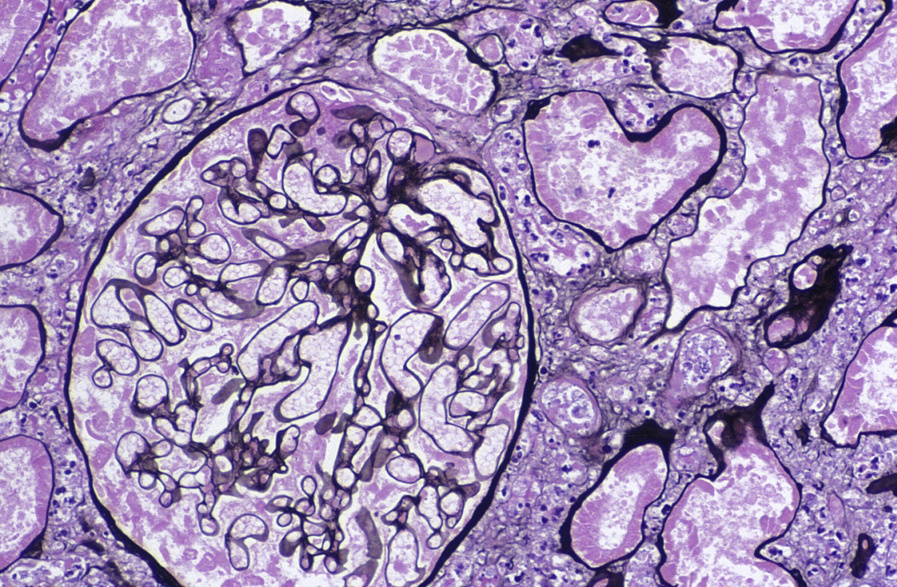
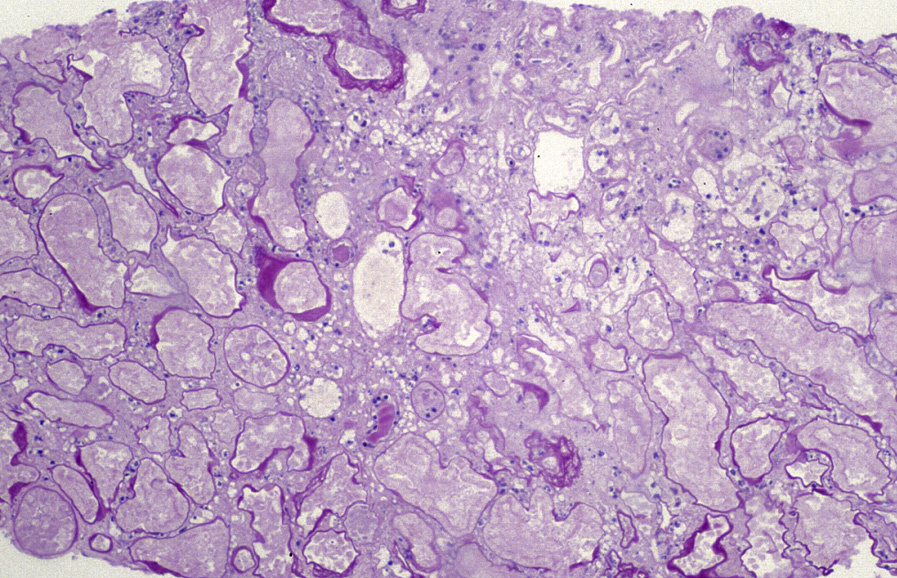
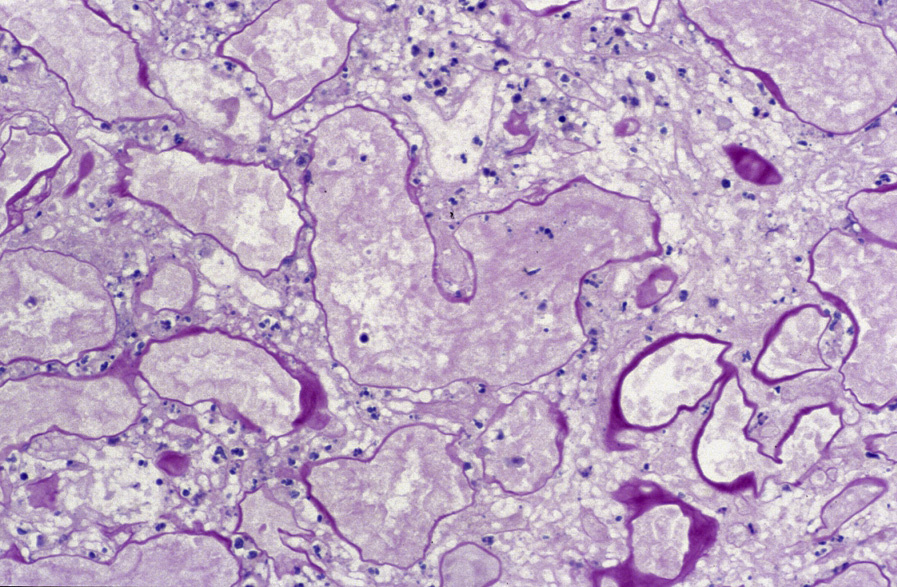
Light microscopy: There is coagulative necrosis involving all tubular segments and glomeruli. Nuclei may be pale and pyknotic, or may no longer be apparent. Thrombi may be present in vessels at the edge of the infarct.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: Widespread necrosis.
Thrombosis of interlobular or larger arteries causes cortical infarcts. Obstetric complications, particularly placental abruption and eclampsia, are common causes. Incidence is decreasing in developed countries as obstetric care is improving.
The extent of necrosis may not be accurately judged from a needle or even wedge biopsy. The kidney may have zones of infarct that are not accurately sampled in a biopsy. Thus, a biopsy cannot distinguish a non-viable kidney, eg, in the transplant setting, from a kidney with a zone of necrosis.