Microscopy Images
Patients are often older, present with oliguric acute kidney injury (AKI), and may have underlying chronic kidney disease (CKD), and have been exposed to high osmolar agents, such as intravenous immunoglobulin (IVIG), high-osmolar radiocontrast agents, or other osmotic agents. Some patients have a history of sepsis and received hydroxyethyl starch as a volume expander. Patients may show low-level proteinuria due to tubular injury and characteristic vacuolated tubular cells on urinalysis. When injury from IVIG is recognized early and therapy is discontinued, nearly all patients recover kidney function, although one-third may need temporary dialysis.
CKD, or end-stage kidney disease when there is preexisting moderate-to-severe kidney disease, may develop. Risk factors for development of osmotic tubular injury are pre-existing CKD, older age, volume depletion, use of diuretics, and exposure to larger amounts of the hyperosmolar agent.
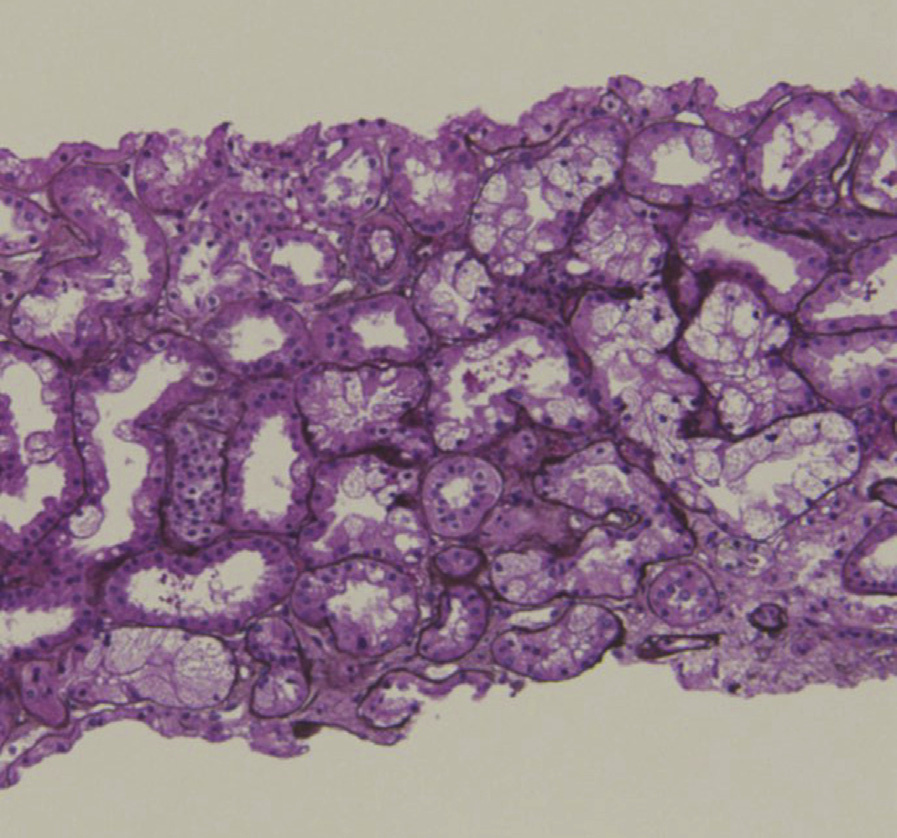
Light microscopy: Tubules show diffuse or focal isometric vacuolization predominantly in the proximal tubules, with clear vacuoles causing luminal narrowing. There may be evidence of underlying CKD. The brush border of the proximal tubules is usually well preserved. Vacuoles are initially small under the luminal cell membrane, with their extent and size increasing gradually.
Immunofluorescence microscopy: No specific staining.
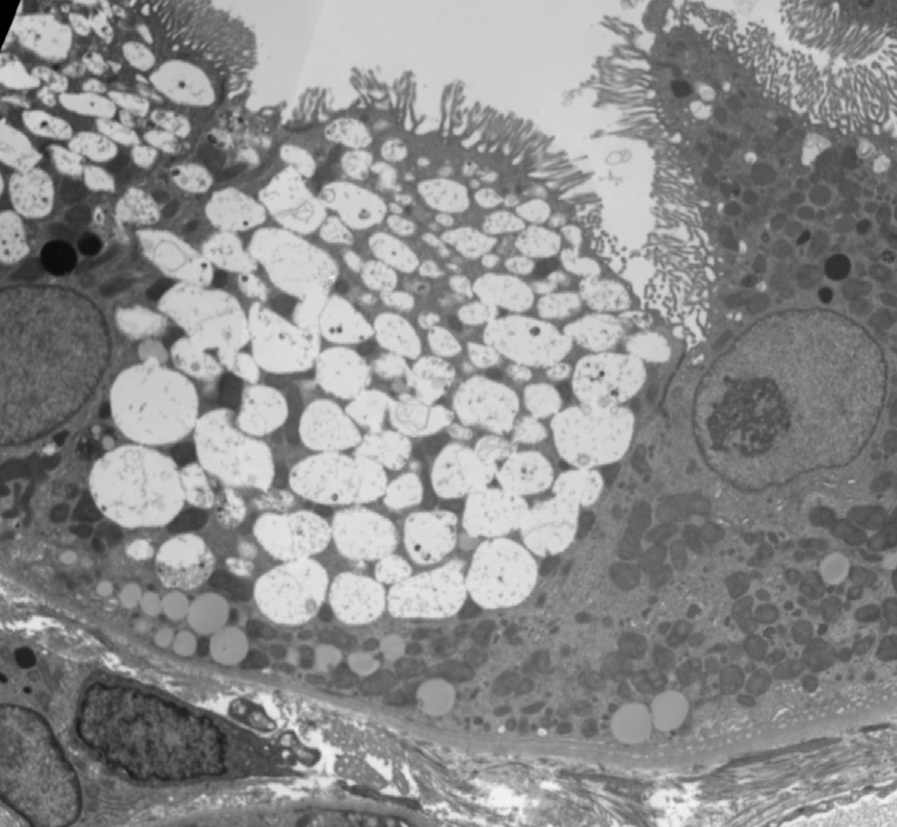
Electron microscopy: The vacuoles can be identified as lysosomes, and typically are empty. In later stages, amorphous or lamellar material may be seen in some of the vacuoles.
Osmotic tubular injury is due to exposure to hyperosmolar agents that are intravenously infused.
Hyperosmolar radiocontrast agents, hydroxyethyl starch, mannitol, and IVIG are common causes of this injury. The macromolecules enter the proximal tubules across the luminal surface, and cause tubular cell swelling before accumulating in lysosomes, visualized as vacuoles by light microscopy. Tubular epithelial cell swelling may contribute to obstruction of the tubular lumen, with decreased urine flow resulting in AKI. IVIG stabilized with sucrose is much more likely to cause this injury than IVIG without sucrose. Proximal tubular cells take up the filtered sucrose via pinocytosis, and these pinocytic vesicles merge to form vacuoles. The vacuoles then fuse with lysosomes, resulting in the characteristic phagolysosomes. The lack of disaccharidase prevents the sucrose from being metabolized, and sucrose accumulation within the cytoplasm creates an osmotic gradient for water entry through the aquaporin 1 channel. Low osmolar or iso-osmolar contrast media is less frequently responsible for osmotic tubular injury.
Calcineurin inhibitor nephrotoxicity can be distinguished by clinical history, and also by electron microscopy, which will reveal dilated endoplasmic reticulum as the cause of vacuolization. In ischemic tubular injury, vacuoles are variable in size and the regenerating-type epithelium shows brush border flattening with blebbing.