Microscopy Images
IgA nephropathy (IgAN) presents with hematuria and varying levels proteinuria, and occurs in all age groups. The incidence of IgAN is much lower in African Americans and highest in the Asian population. The progression of disease can be rapid, especially in those with crescents. Approximately one-third of patients progress to kidney failure over time. IgAN recurs in kidney transplants in up to 60% of patients, but rarely results in graft loss. Henoch-Schönlein purpura also has mesangial IgA deposition and is morphologically similar to IgAN; however, crescents are more frequently present in biopsied Henoch-Schönlein purpura than IgAN.
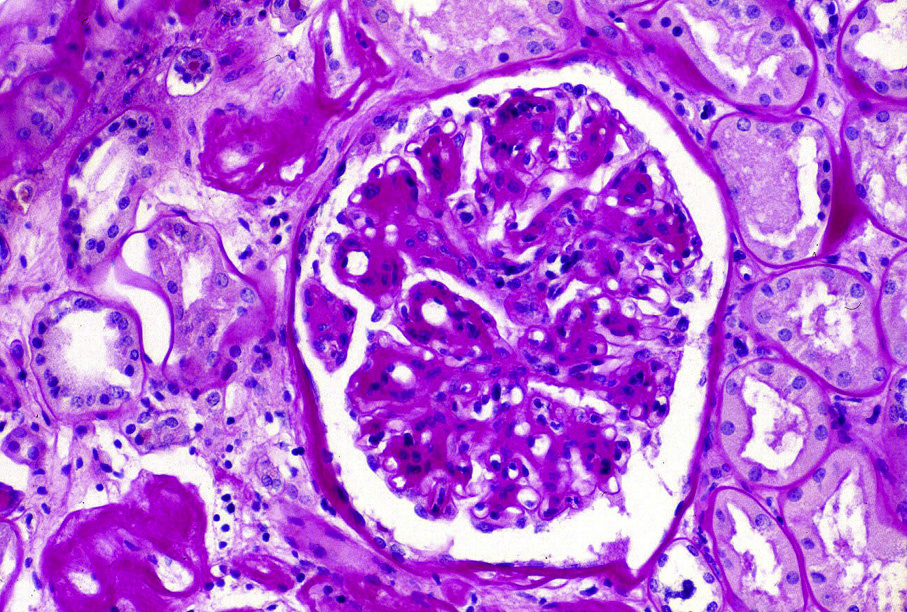
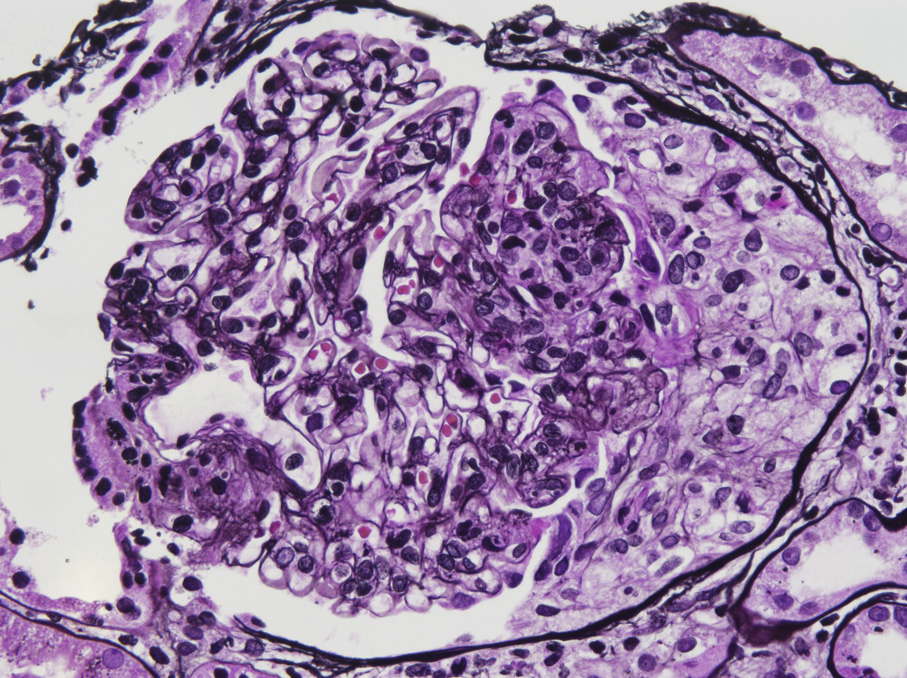
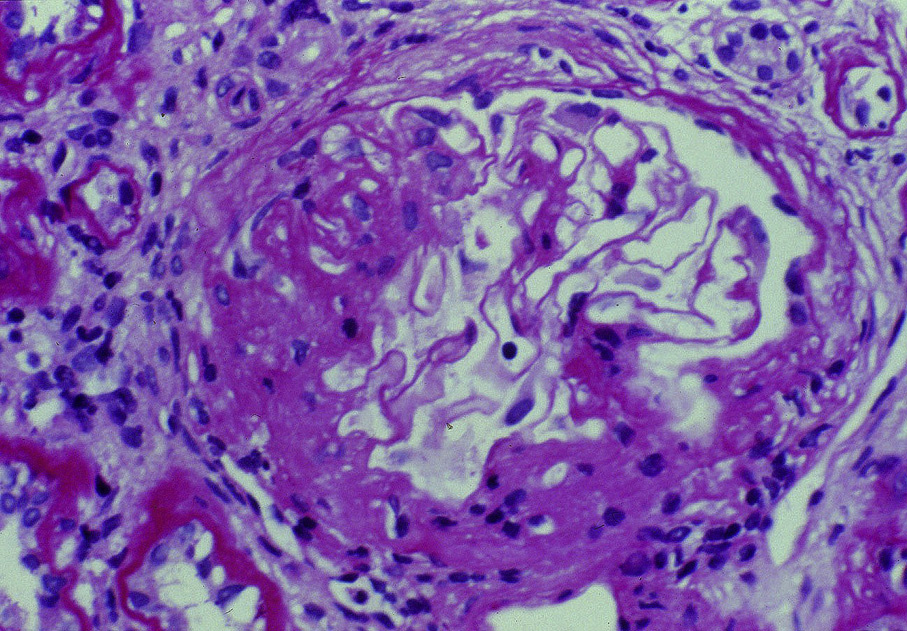
Light microscopy: Variable presentation from minimal mesangial expansion to diffuse proliferation; may have sclerosis and/or crescents. Morphologic markers for worse prognosis identified by the Oxford IgAN classification include significant mesangial proliferation, any segmental sclerosis or adhesion, any endocapillary hypercellularity lesion, and tubulointerstitial fibrosis >25%.
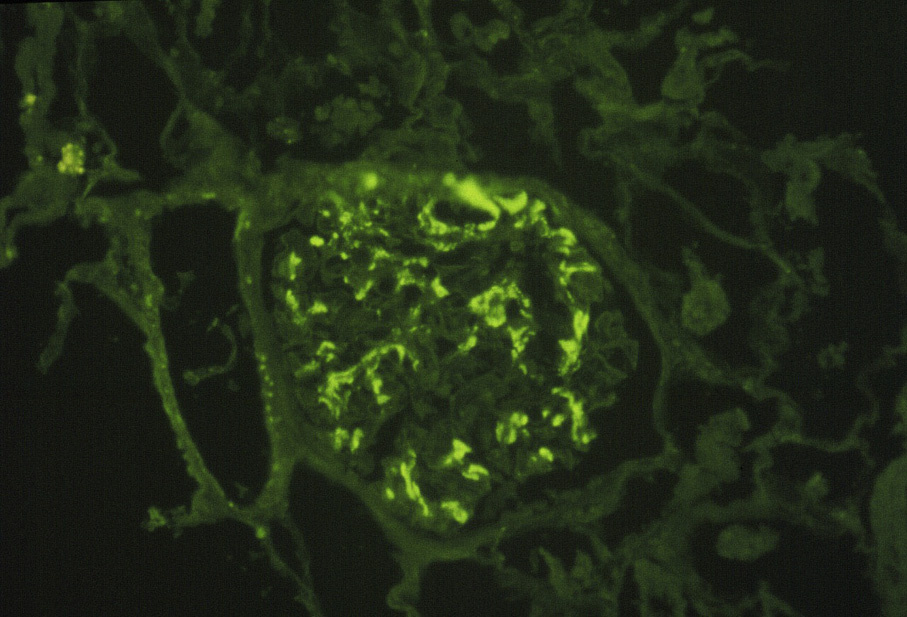
Immunofluorescence microscopy: Dominant or codominant IgA mesangial staining with variable IgG and IgM. C3 is often present, usually equal or less than IgA staining. Deposits are polyclonal, often with λ light chains slightly more intense than κ light chains.
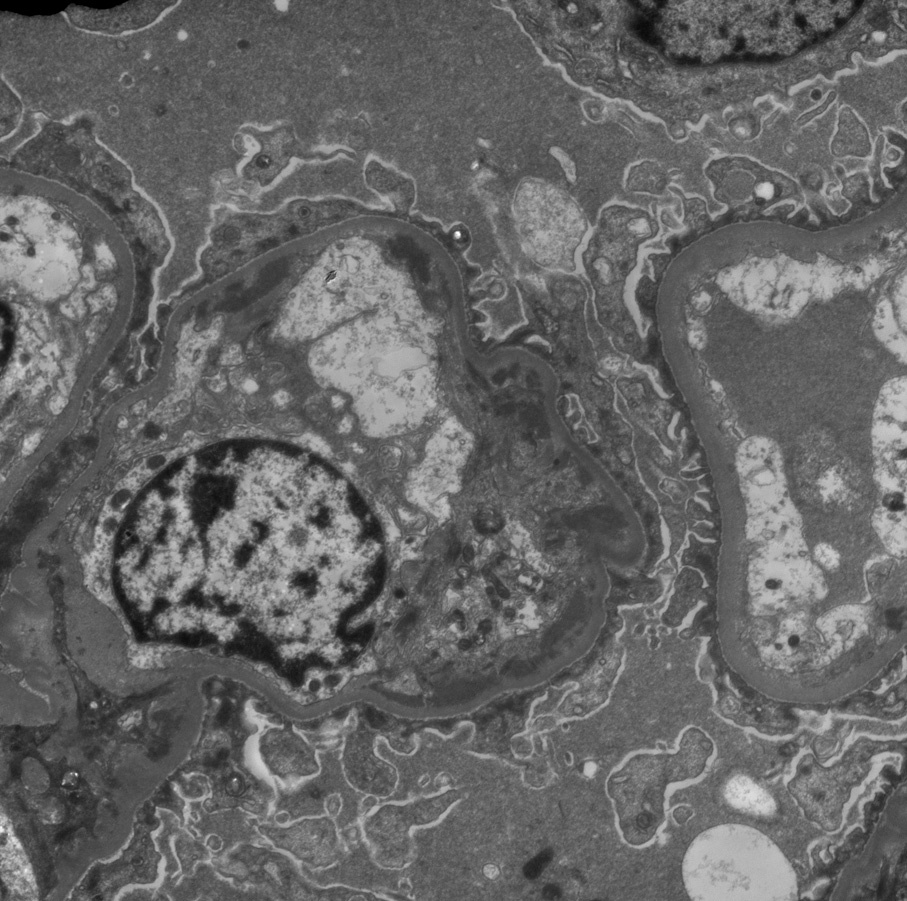
Subendothelial deposits are often present when there is endocapillary hypercellularity.
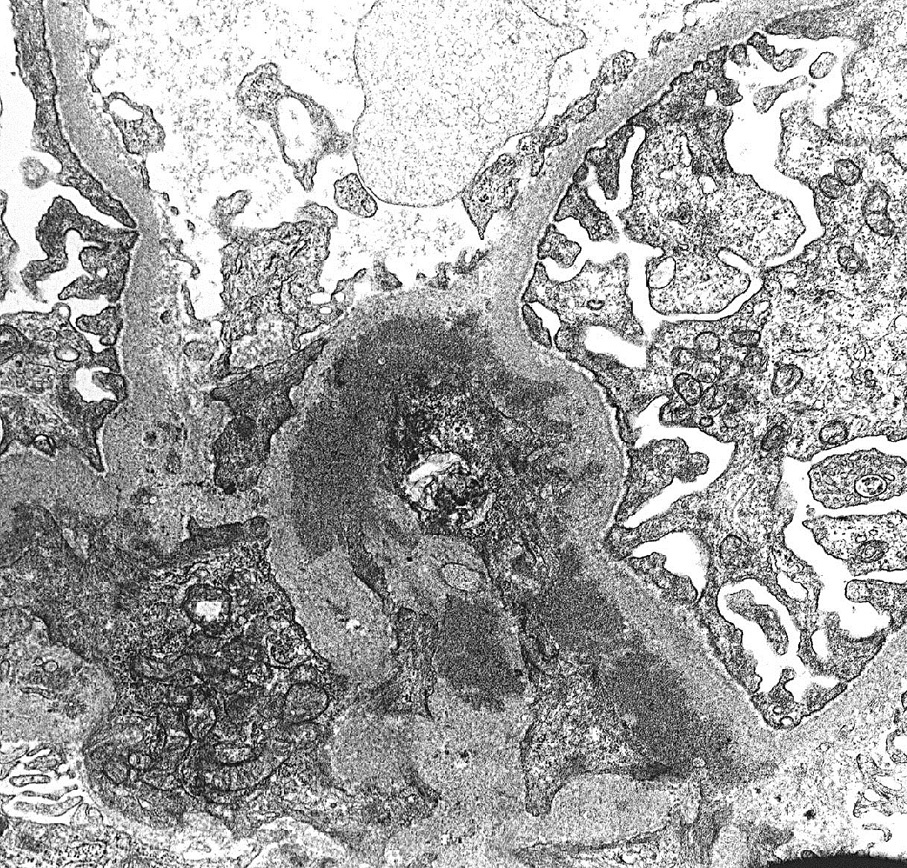
Electron microscopy: Mesangial deposits with increased mesangial matrix and cellularity. Subendothelial deposits may also be present, particularly in more active disease with endocapillary hypercellularity.
Antigenic galactose-deficient hinge region IgA1 plays a central role in the pathogenesis of IgAN. IgG or IgA antibodies form immune complexes with aberrantly glycosolated IgA1 leading to glomerular deposition.
Morphologic clues to the diagnosis of IgA dominant postinfectious glomerulonephritis versus IgAN include endocapillary hypercellularity with neutrophils by light microscopy, C3 greater than IgA staining by immunofluorescence, and subepithelial hump-like deposits by electron microscopy.