Microscopy Images
Patients with dense deposit disease (DDD) usually present with nephrotic/nephritic syndrome, hypertension, and reduced glomerular filtration rate. Serum C3 levels are typically decreased with normal serum C4.
Progression to kidney failure is common, usually within 10 years. Older patient age, lower glomerular filtration rate, and the presence of subepithelial humps are predictors of rapid disease progression. DDD has a high rate of recurrence in the transplant.
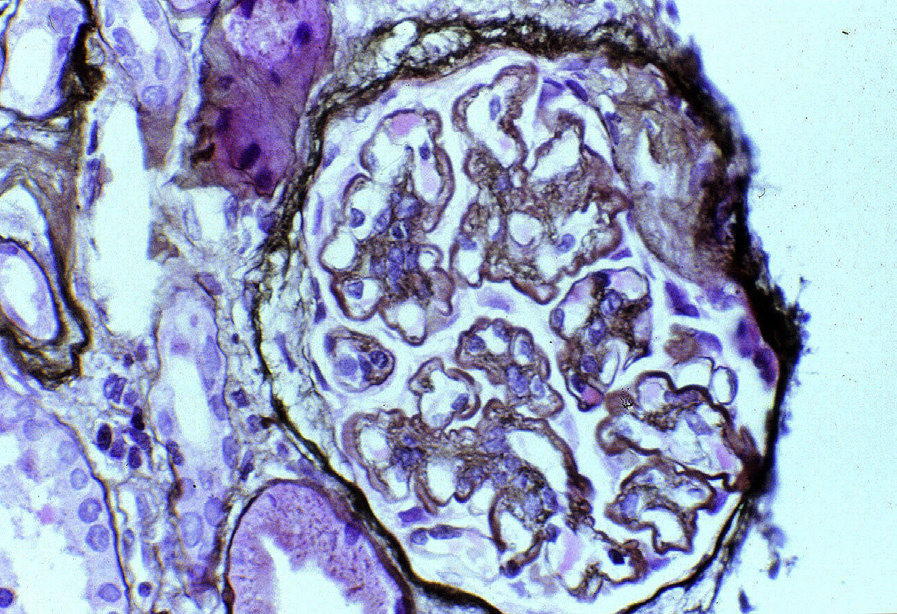
Light microscopy: The glomeruli show variable patterns of injury, including mesangial proliferation or a membranoproliferative pattern with double contours of glomerular basement membranes (GBMs).
Cellular interposition in the GBM occurs without the eosinophilic appearance typical of immune complex deposits. A refractile, ribbon-like appearance and weak or absent silver staining of the GBMs are clues to DDD. Crescents may be present.
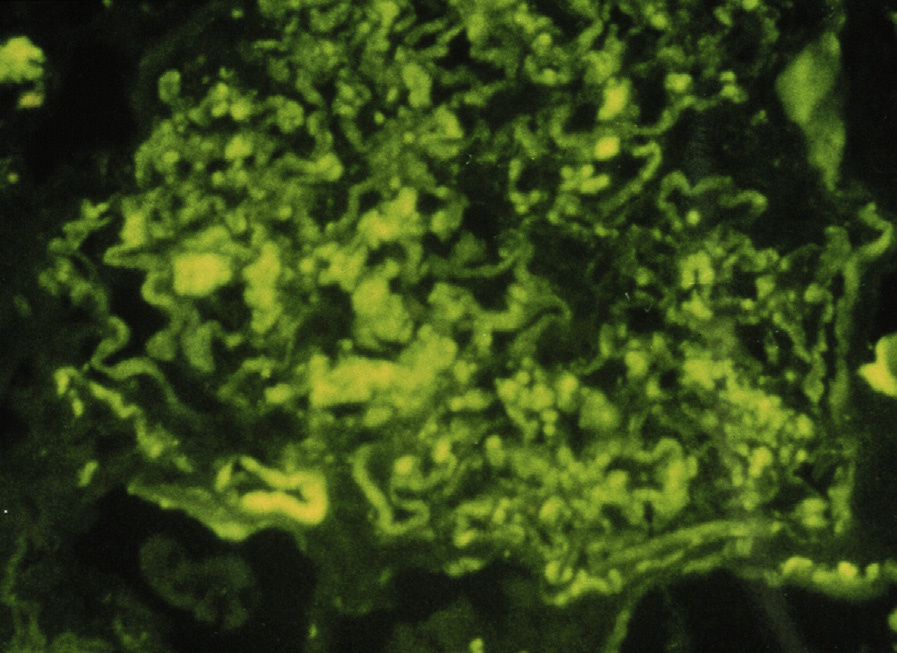
Immunofluorescence microscopy: Dominant (at least 2 intensity steps more than immunoglobulins) or only C3 staining with occasional globular mesangial and irregular, segmental capillary wall pattern, often sausage-like in appearance.
Limited segmental immunoglobulin staining, immunoglobulin M, or less often immunoglobulin G, may be present.
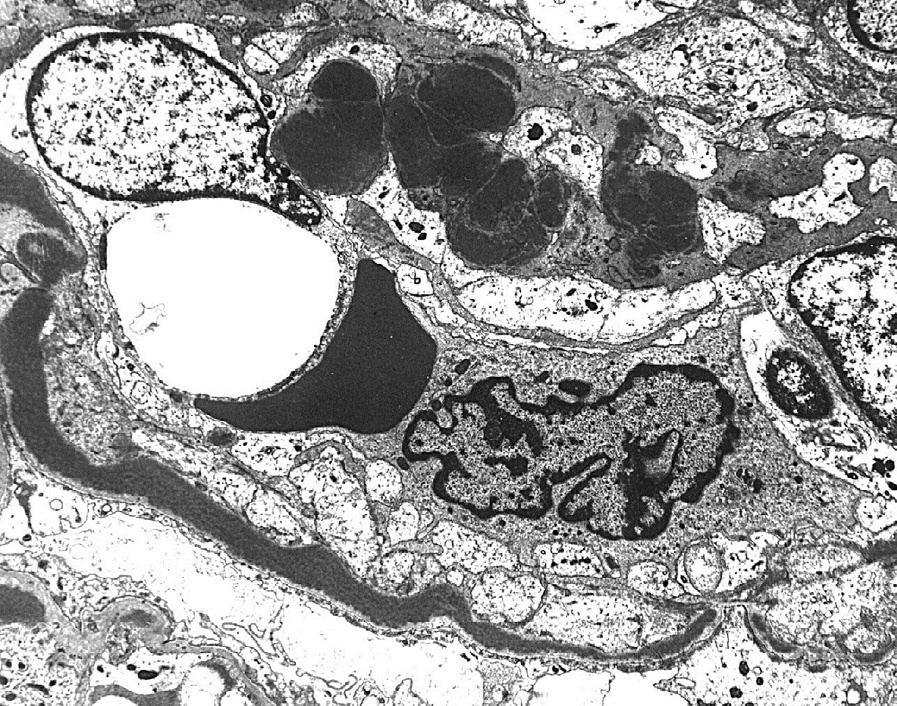
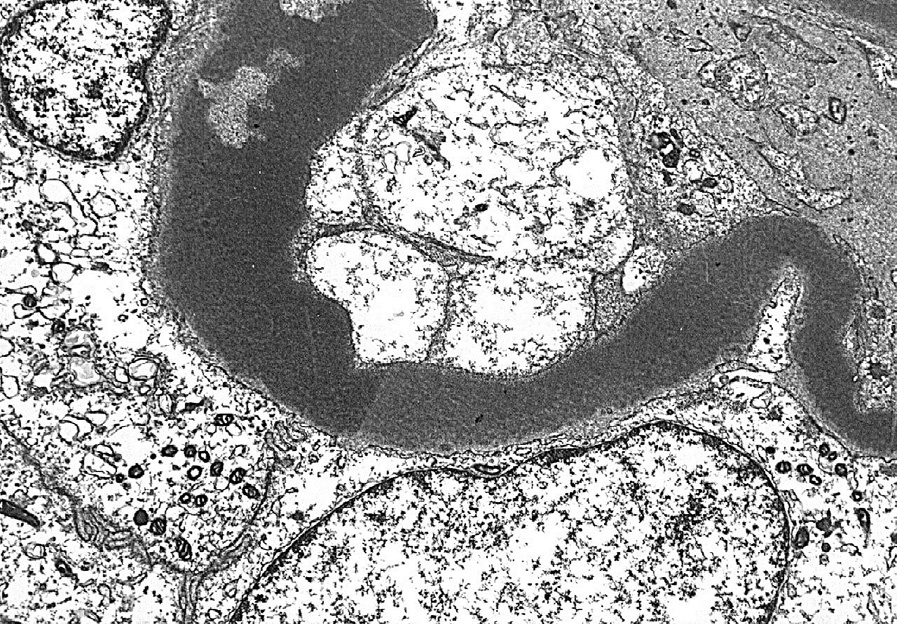
Electron microscopy: Dense transformation of the basement membrane lamina densa, which may also be found in tubular basement membranes and Bowman’s capsule. Mesangial dense globular deposits are often present.
Abnormalities in the regulation of the alternative complement pathway are due to increased C3 convertase activation. Possible pathogenesis includes C3 nephritic factor (C3Nef), an autoantibody which stabilizes C3 convertase C3bBb, or factor H deficiency or inactivation with decreased decay of C3bBb.
Glomerulonephritis with dominant C3 also shows dominant or only C3 by immunofluorescence; however, deposits do not show the dense transformation of DDD, and are mainly subendothelial and mesangial.
Other entities with a membranoproliferative pattern of injury (eg, lupus nephritis, IgA nephropathy with proliferation, and postinfectious glomerulonephritis) show disease-specific immunofluorescence findings and absence of dense transformation of the GBMs.