Microscopy Images
Membranoproliferative glomerulonephritis (MPGN) is a lesion caused by subendothelial immune complex deposits. Patients are typically children or young adults, or older adults with chronic infections, and usually present with mixed nephrotic/nephritic syndrome, and decreased complement C3. The lesion is characterized by mesangial and endocapillary proliferation and double contours of the glomerular basement membrane (GBM) on silver stain. Similar light microscopic appearances may be seen in class IV diffuse lupus nephritis, cryoglobulinemic glomerulonephritis (GN), proliferative GN with monoclonal deposits, fibrillary GN, and C3 glomerulopathies, all with distinct immunofluorescence and/or electron microscopic appearances. Double contours of GBMs are also present in conditions with chronic endothelial injury, including chronic thrombotic microangiopathy, transplant glomerulopathy, and preeclampsia. Patients with MPGN often have progressive decline in kidney function, with 50% kidney survival at 10 years. MPGN recurs in the transplant in about 30% of cases.
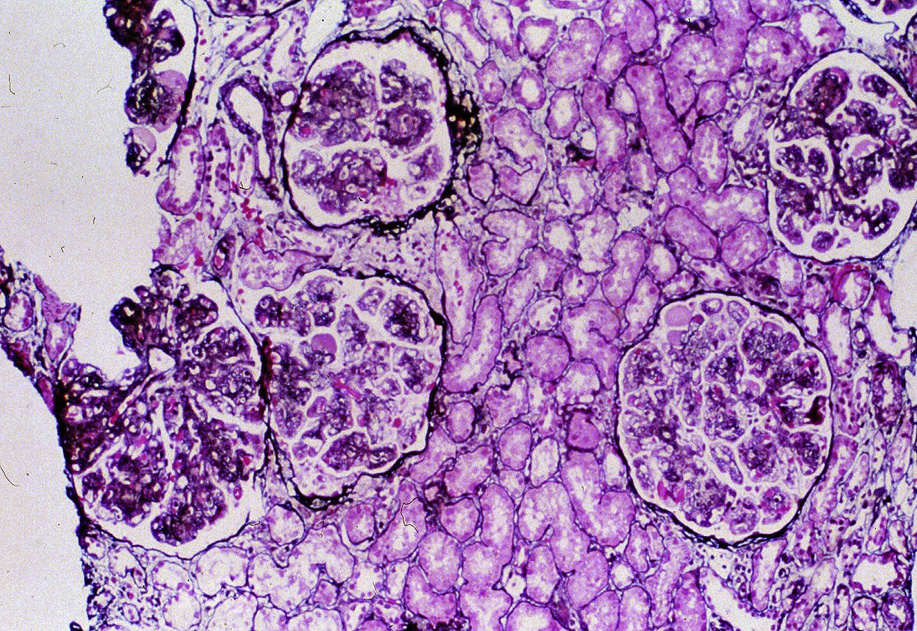
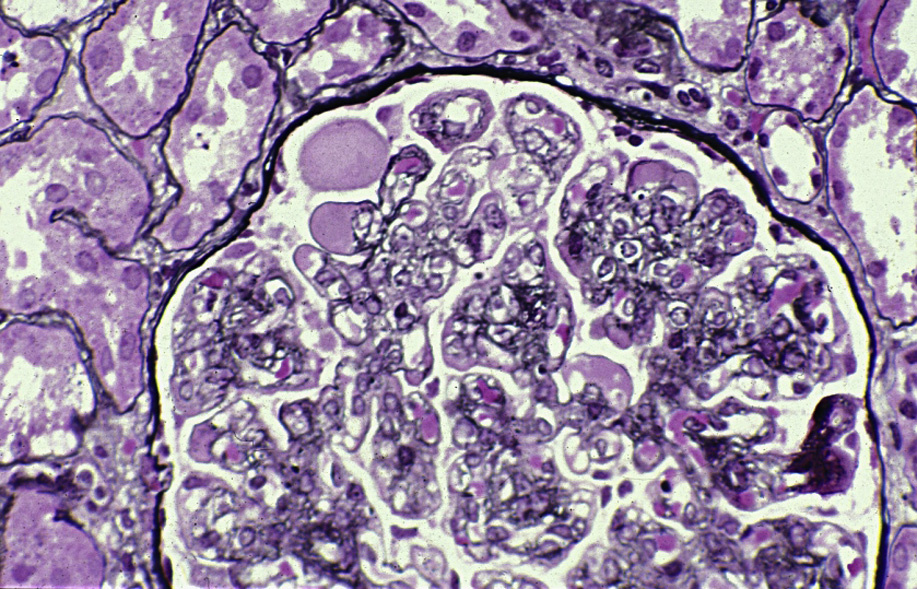
Light microscopy: There is endocapillary proliferation, often diffuse and global, with double contours of GBM on silver stain. Crescents may be present.
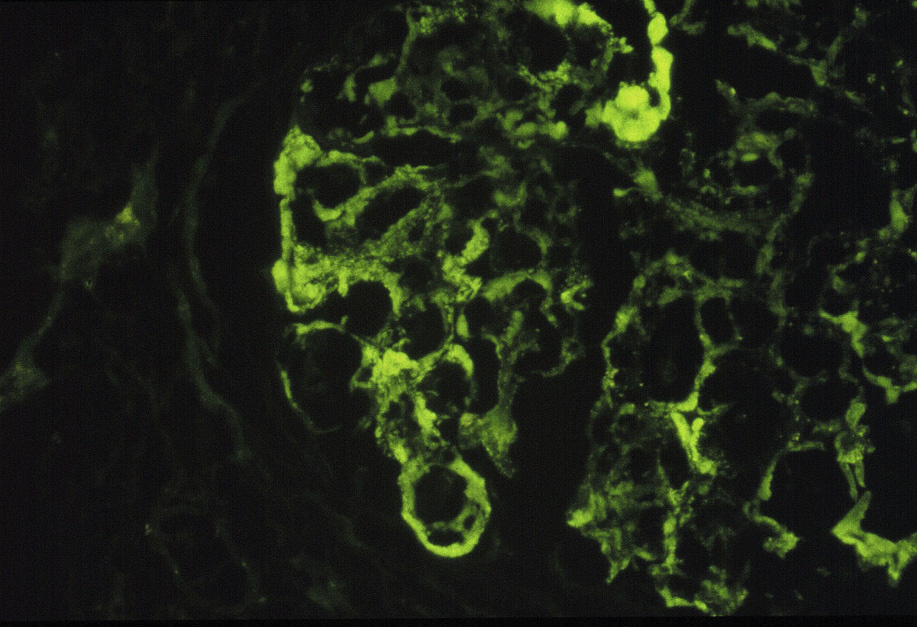
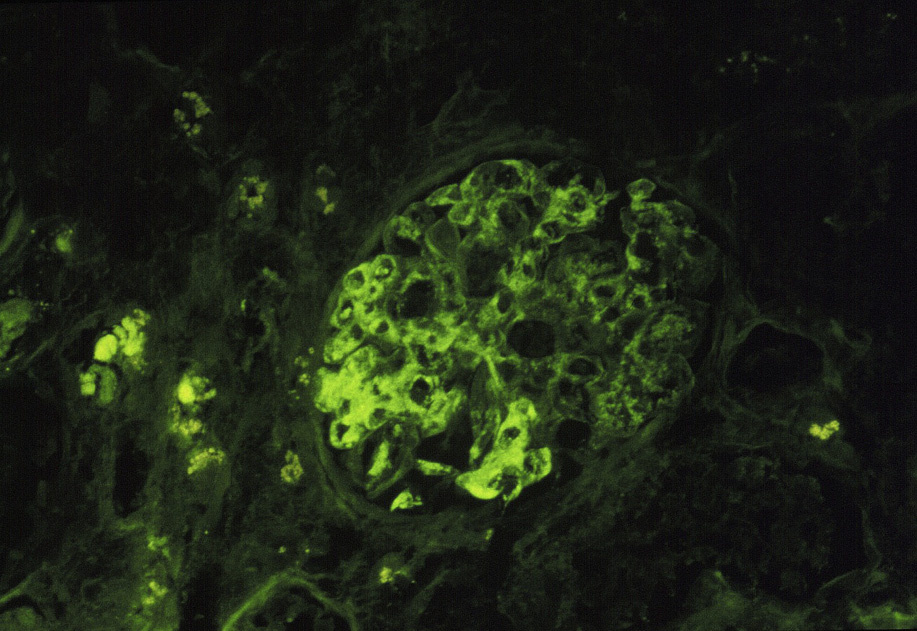
Immunofluorescence microscopy: Mesangial and chunky, irregular capillary wall deposits, some sausage-shaped due to molding under the GBM, of polyclonal immunoglobulin G (IgG), C3, and often C1q.
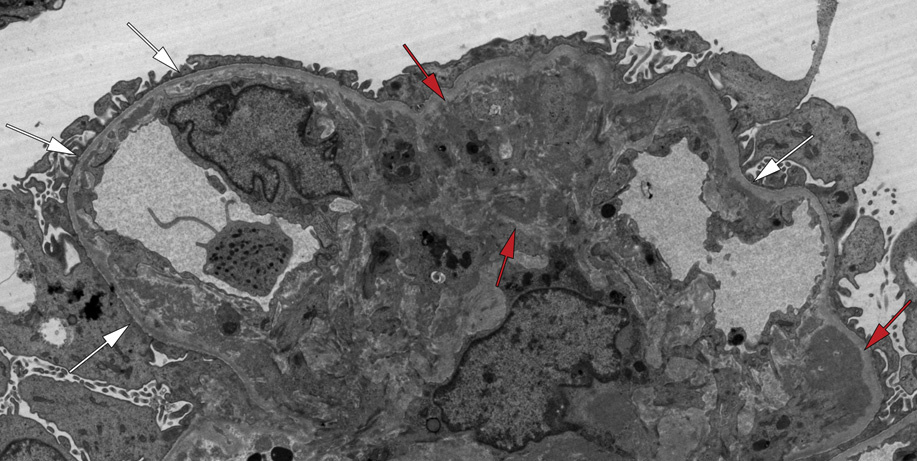
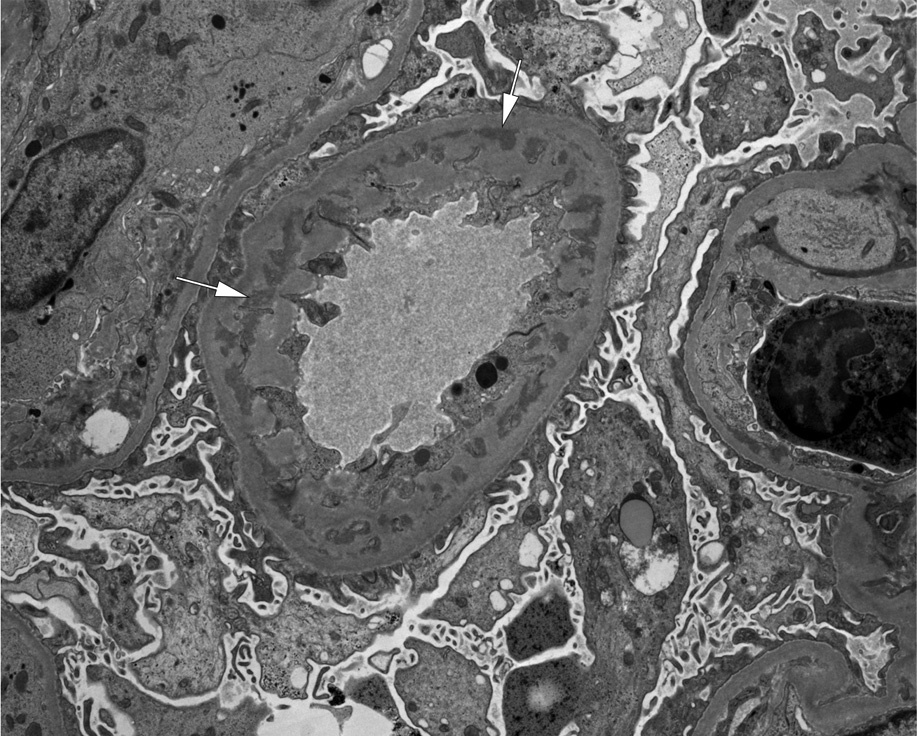
Electron microscopy: Subendothelial and mesangial deposits with interposed cells along the GBM, double contours with new GBM formation underneath subendothelial deposits, extensive foot process effacement, and endocapillary proliferation.
MPGN is due to subendothelial and mesangial deposits, and may occur due to chronic infections, such as hepatitis C. Specific morphologic appearances may allow diagnosis of other specific etiologies, such as C3 glomerulopathy, cryoglobulinemic GN, or monoclonal protein underlying the light microscopic appearance.
MPGN-type lesions may occur due to cryoglobulins (IgM dominance, often clonal shift with unequal κ vs λ light chains, substructured deposits shown by electron microscopy); fibrillary GN (polyclonal IgG, fibrils by electron microscopy); amyloid (more acellular, fibrils by electron microscopy, Congo Red positive); C3 glomerulopathies (C3 with no or minimal immunoglobulin by immunofluorescence, dense deposits in dense deposit disease); proliferative GN with monoclonal deposits (monoclonal by immunofluorescence); diffuse lupus nephritis (“full-house” staining with IgG, IgA, IgM, C3, and C1q by immunofluorescence, reticular aggregates by electron microscopy).