Agnes B. Fogo, MD, Mark A. Lusco, MD, Behzad Najafian, MD, and Charles E. Alpers, MD
AJKD Atlas of Renal Pathology
Microscopy Images
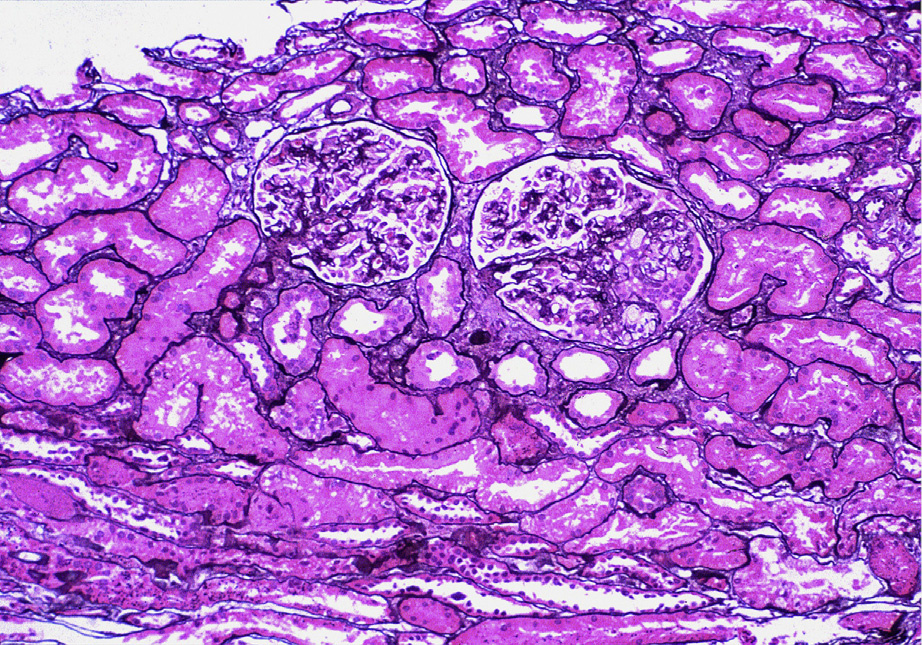
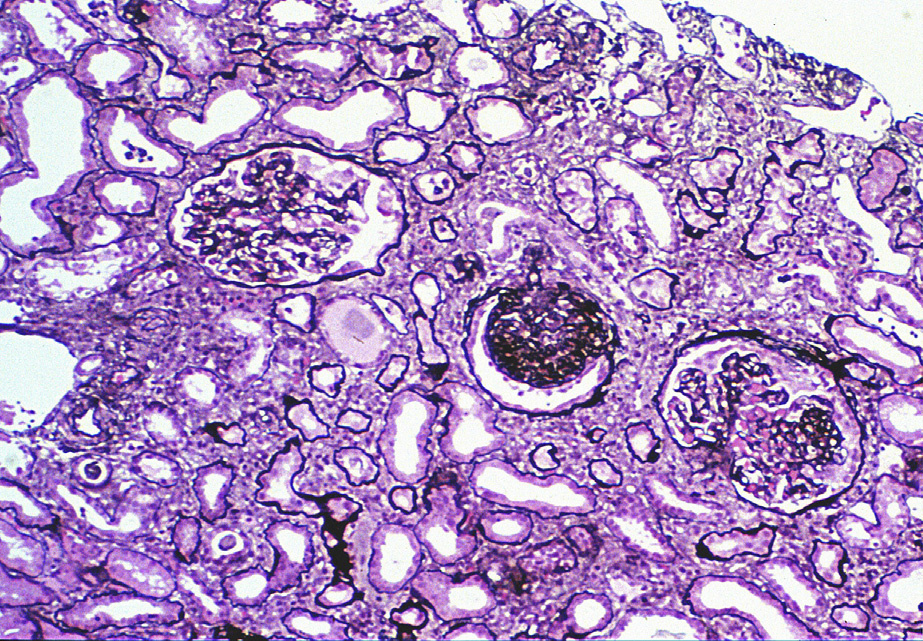
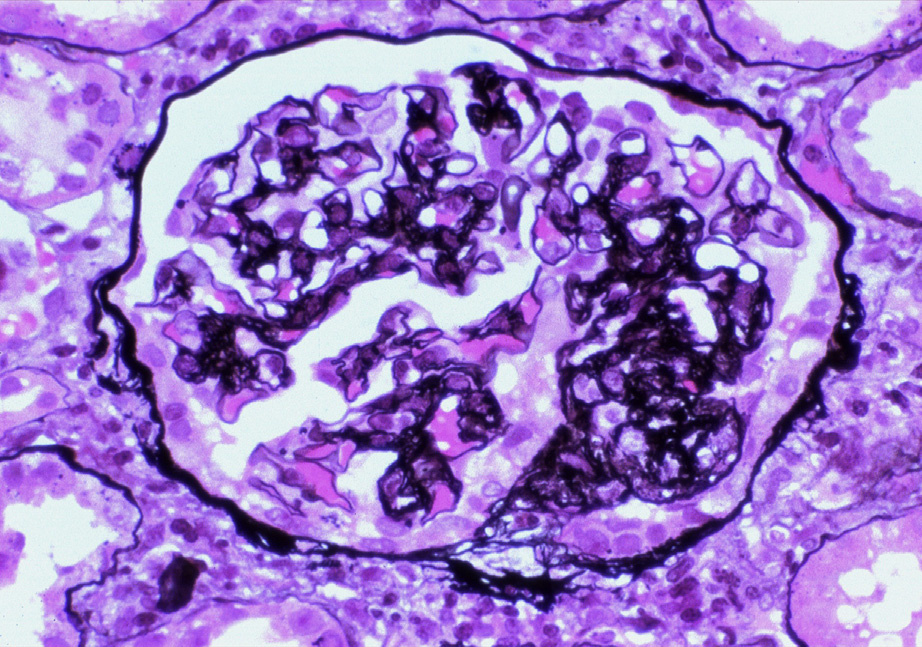
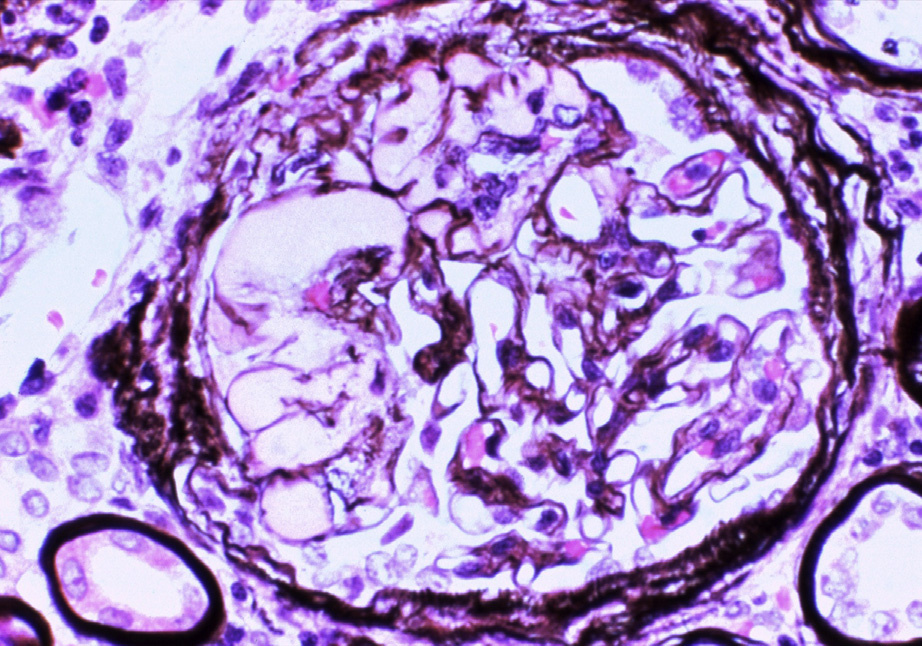
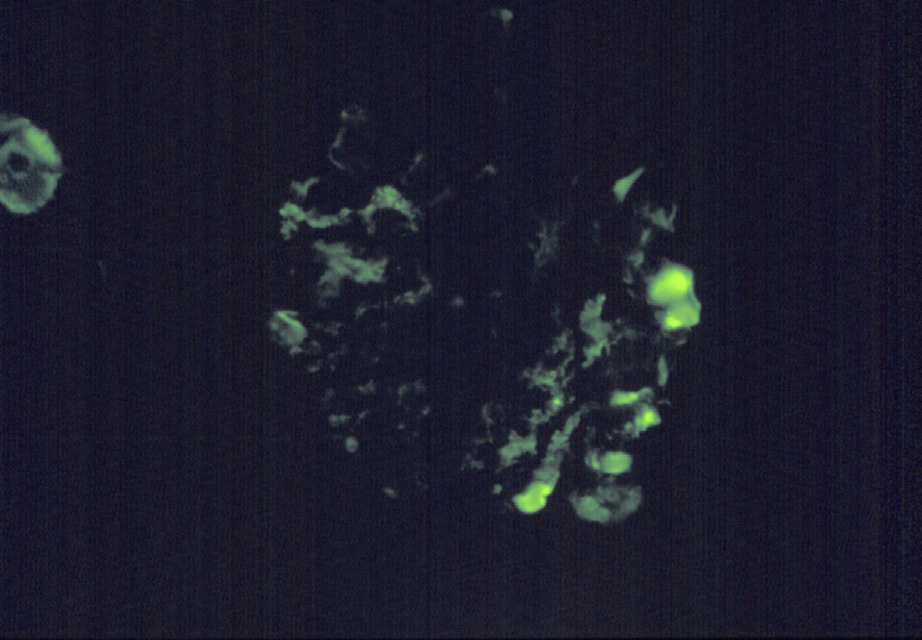
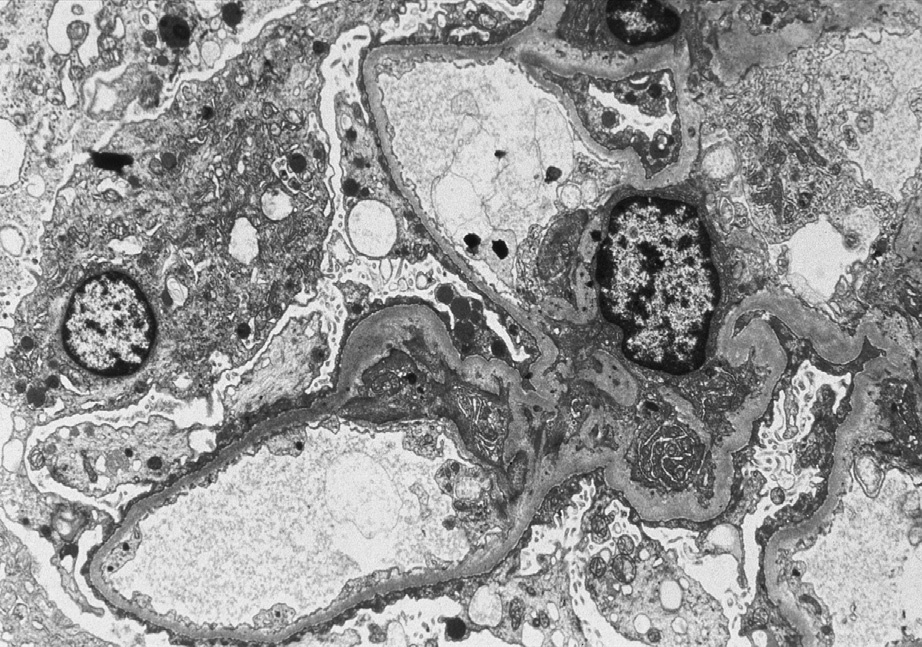
Figure 1. Two small peripheral foci of segmental sclerosis with intracapillary foam cells and prominence of overlying visceral epithelial cells (right glomerulus), with normal left glomerulus by light microscopy, representative of an early segmental sclerosing lesion in focal segmental glomerulosclerosis, not otherwise specified variant (Jones silver stain). Reproduced with permission from AJKD 33(4):e1.Figure 2. More advanced lesions of focal segmental glomerulosclerosis, not otherwise specified (NOS) variant. The central glomerulus shows global sclerosis; the right glomerulus shows peripheral segmental sclerosis, NOS; and the left glomerulus shows no lesion by light microscopy. There is moderate interstitial fibrosis and tubular atrophy (Jones silver stain). Reproduced with permission from AJKD 33(4):e1.Figure 3. This segmental sclerotic lesion is composed of obliteration of capillary lumens by increased matrix with overlying activated hypertrophic, but not proliferating, visceral epithelial cells, diagnostic of focal segmental glomerulosclerosis, not otherwise specified variant. The remaining left portion of the glomerular tuft appears unremarkable (Jones silver stain). Reproduced with permission from AJKD 33(4):e1.Figure 4. Hyalinosis and segmental sclerosis in focal segmental glomerulosclerosis, not otherwise specified variant. Hyaline is defined as smooth glassy-appearing material, resulting from insudation of plasma proteins (Jones silver stain). Reproduced with permission from AJKD 33(4):e1.Figure 5. Immunoglobulin M (IgM) or C3 staining in mesangial areas in focal segmental glomerulosclerosis, not otherwise specified variant. This may also occur in areas of hyalinosis. Although these may be associated with small areas of electron density by electron microscopy (not shown), immune complex densities are not typically found (immunofluorescence microscopy, IgM). Reproduced with permission from AJKD 33(4):e1.Figure 6. The mesangial matrix is mildly increased, endothelial cells are unremarkable, and podocytes show extensive blunting and effacement of foot processes with early microvillous transformation. There are no immune complex deposits (electron microscopy). Reproduced with permission from AJKD 33(4):e1.
Clinical & Pathologic Features
Focal segmental glomerulosclerosis (FSGS) is characterized by nephrotic syndrome and has exceeded membranous nephropathy as the most common cause of nephrotic syndrome in adults in the United States.
FSGS presents similarly to minimal change disease, but is not usually responsive to steroid therapy and has progressive glomerular filtration rate loss.
Light microscopy: FSGS pattern of scarring.
Immunofluorescence microscopy: No or limited deposits (nonspecific immunoglobulin M and C3 staining in sclerotic areas).
Electron microscopy: Extensive foot process effacement. No or limited deposits.
Etiology / Pathogenesis
Undefined circulating factor(s) that mediate abnormal glomerular permeability lead to segmental sclerosis in primary FSGS, with podocyte injury and dedifferentiation.
Secondary FSGS can occur in other non–immune complex disease (eg, arterionephrosclerosis and reflux/ chronic pyelonephritis nephropathy). It is seen in the chronic stage of vasculitic injury or immune complex diseases.
Differential Diagnosis
In a small biopsy sample with surrogate markers of possible unsampled FSGS (ie, glomerulomegaly and interstitial fibrosis in a young patient) and extensive foot process effacement in the absence of diagnostic segmental lesion, FSGS cannot be distinguished from minimal change disease.
Limited (,50%) foot process effacement favors a secondary etiology, except in patients with treatment and partial response before biopsy. In secondary FSGS, extensive foot process effacement may occur, particularly in segmentally sclerosed glomeruli.
Perihilar variant of FSGS is usually of secondary etiology.
Significant immune complex deposits by immunofluorescence and electron microscopy indicate a secondary etiology.