Microscopy Images
Clinical manifestations are heterogeneous. Classic cases present with peripheral neuropathy, skin vascular dilatations (angiokeratoma corporis diffusum), corneal opacities, abdominal pain and diarrhea, arrhythmias, ventricular hypertrophy, strokes, and kidney failure.
The initial clinical manifestations of kidney involvement are microalbuminuria and proteinuria, which may start in the teenage years. This is followed by progressive glomerular filtration rate decline. Untreated patients (especially men) develop end-stage renal disease in their 40s and 50s.
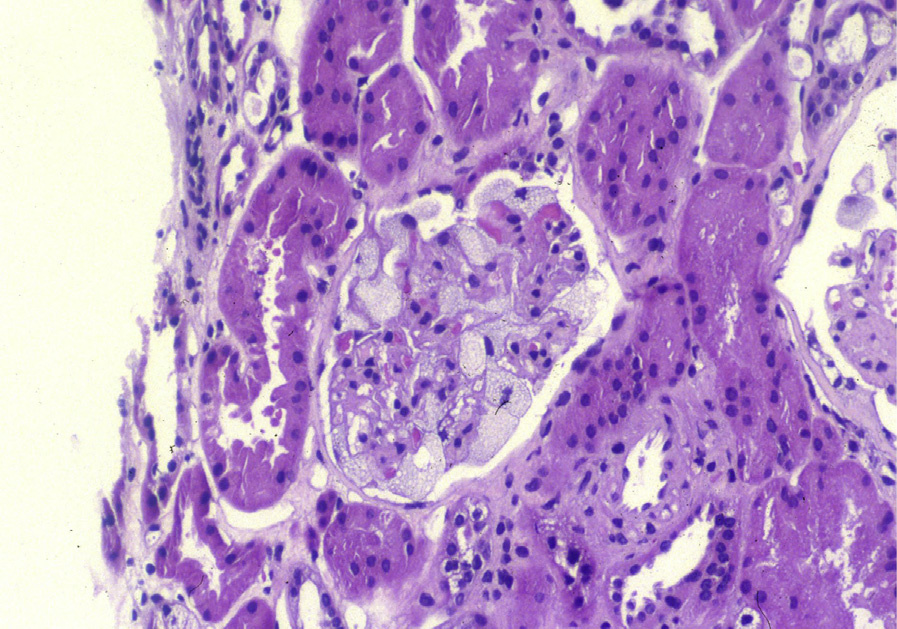
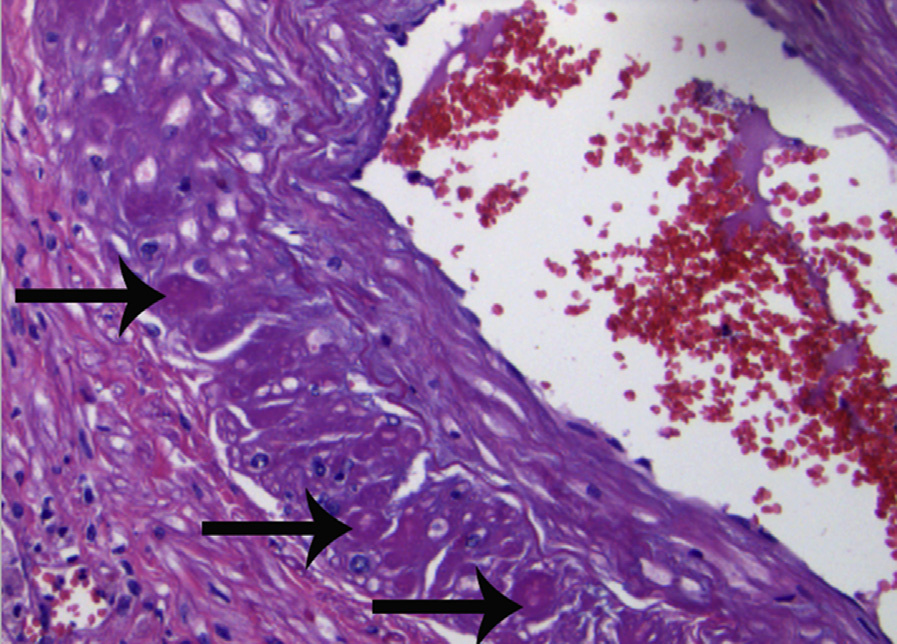
Light microscopy: The characteristic accumulated glycosphingolipid (GSL) inclusions are removed during tissue processing for paraffin embedding. Therefore, the cells, especially podocytes, parietal epithelial cells, and distal tubular epithelial cells, appear vacuolated. Hyaline-like material accumulates in the media of arteries and arterioles (Fabry arteriopathy) and sometimes in the mesangial regions.
Immunofluorescence: Negative.
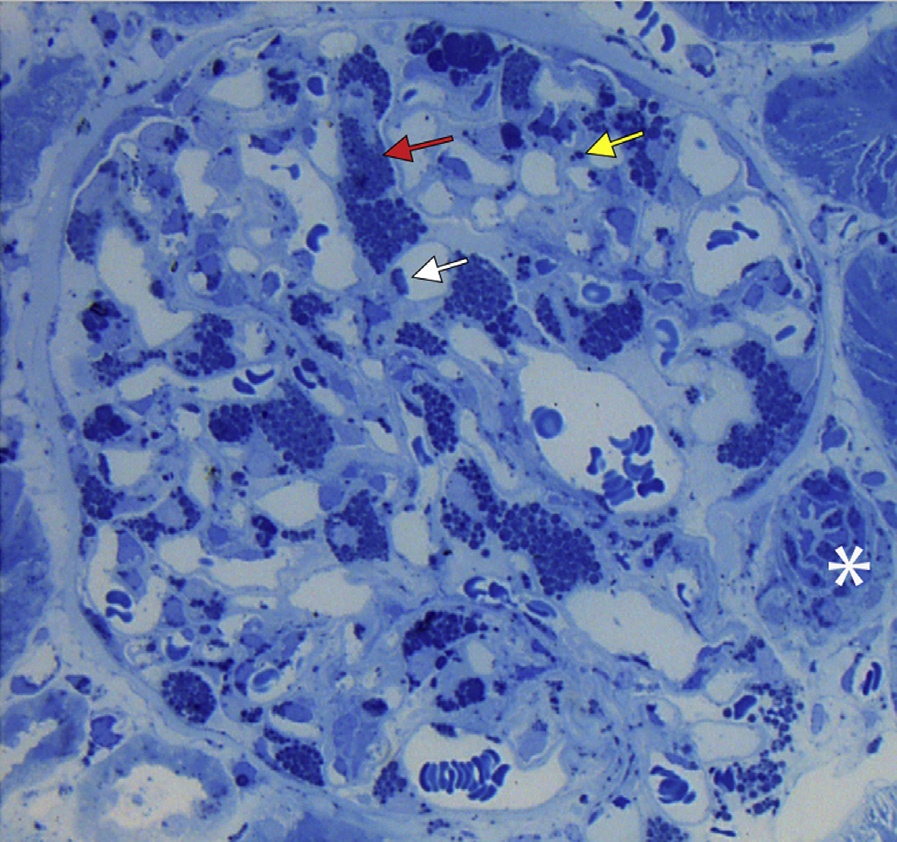
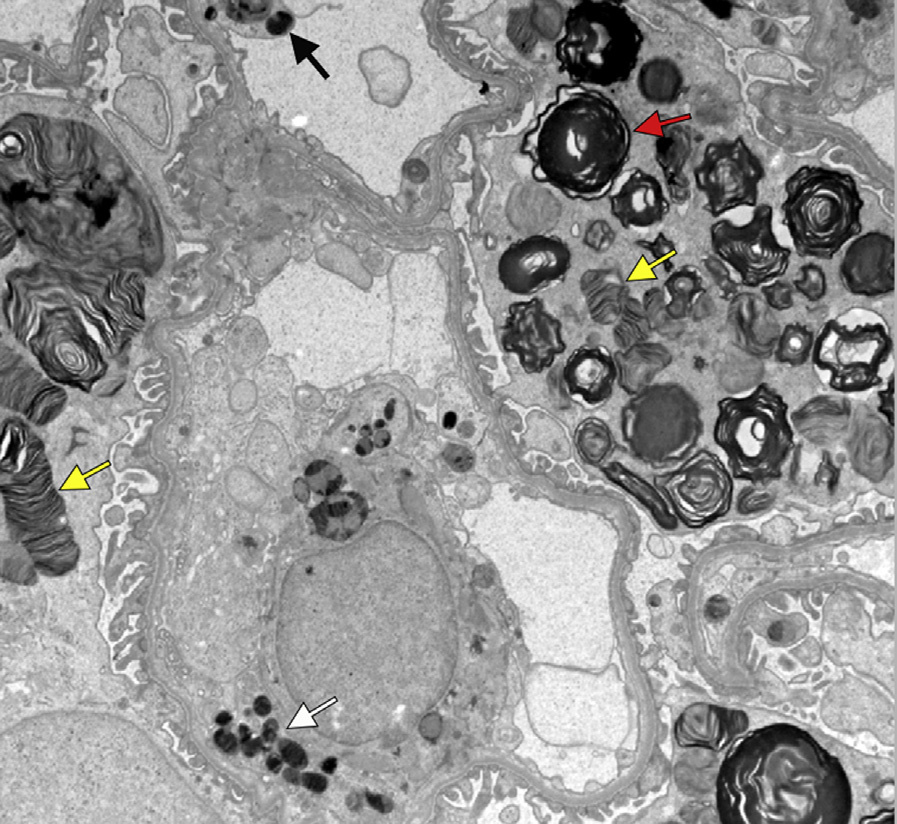
Electron microscopy: Highly electron-dense multilamellar inclusions of GSL (myelin figures made of concentric layers and zebra bodies, which have elongated striped appearance) are present in various cell types. The inclusions also stain darkly by toluidine blue on semi-thin sections. Abundant inclusions are present in podocytes, parietal epithelial cells, and distal tubular cells. Mesangial and endothelial cell inclusions may not be present in patients treated with enzyme replacement therapy or in women who are disease carriers. Arteries and arterioles show inclusions in smooth muscle cells and hyaline-like material, consistent with Fabry arteriopathy.
Fabry disease is an X-linked lysosomal storage disease due to deficiency of alpha-galactosidase A.
This results in accumulation of GSLs, especially globotriaosylceramide (GL3), in the form of intralysosomal inclusions.
Cytoplasmic inclusions similar to Fabry inclusions can also be seen in iatrogenic phospholipidosis secondary to amphophilic drugs, such as chloroquine, amiodarone, and hydroxychloroquine. Foamy podocytes by light microscopy can also be seen in other lysosomal storage diseases. However, inclusions in those conditions appear different from Fabry inclusions by electron microscopy.