Microscopy Images
Fibrillary glomerulonephritis occurs mainly in adults with an average age of around 50 years. It presents with nephrotic syndrome, hematuria, and reduced glomerular filtration rate in about two-thirds of patients. Nearly half of patients progress to endstage kidney disease within 2 to 4 years. Recurrence in allograft kidneys developed in 36% of patients in one small series.
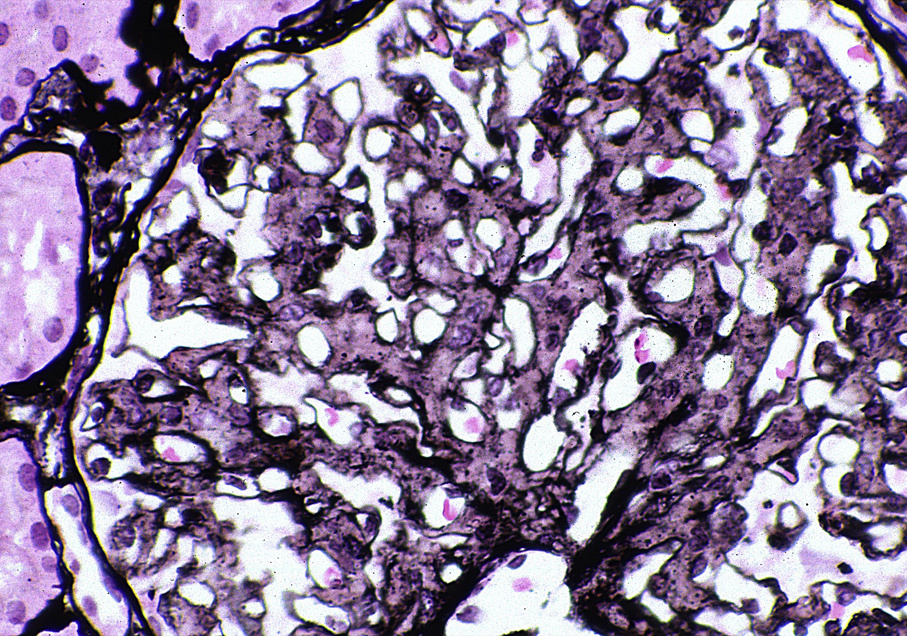
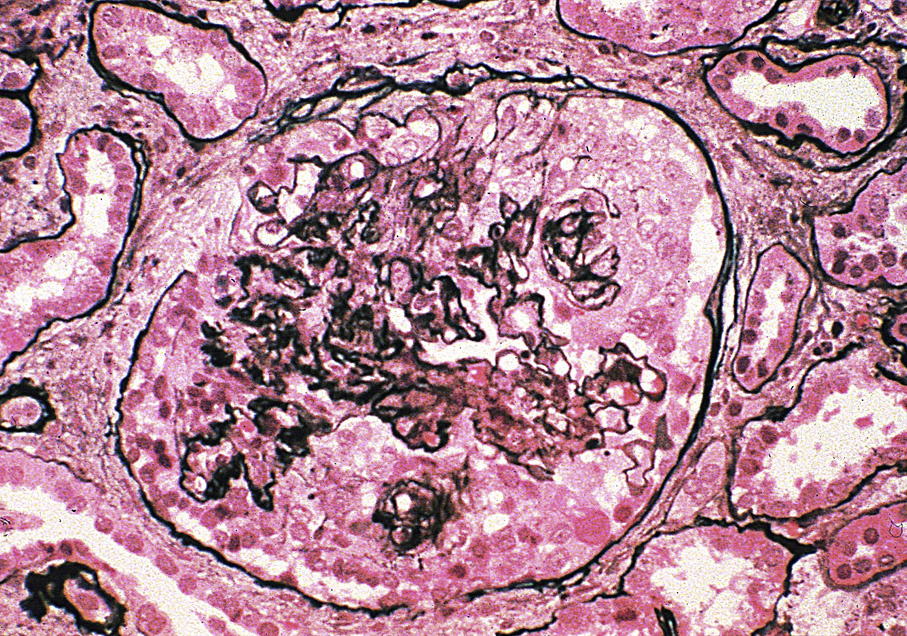
Light microscopy: Variable appearance, but commonly with mesangial expansion due to infiltrating extracellular material and frequent lobular membranoproliferative appearance with glomerular basement membrane (GBM) thickening. Diffuse mesangial or endocapillary proliferation is seen, with crescents present in 17% to 31% of cases (but usually involving a minority of glomeruli in an individual case), and variable glomerulosclerosis. A membranous pattern with spikes is occasionally present. Congo red stain is negative.
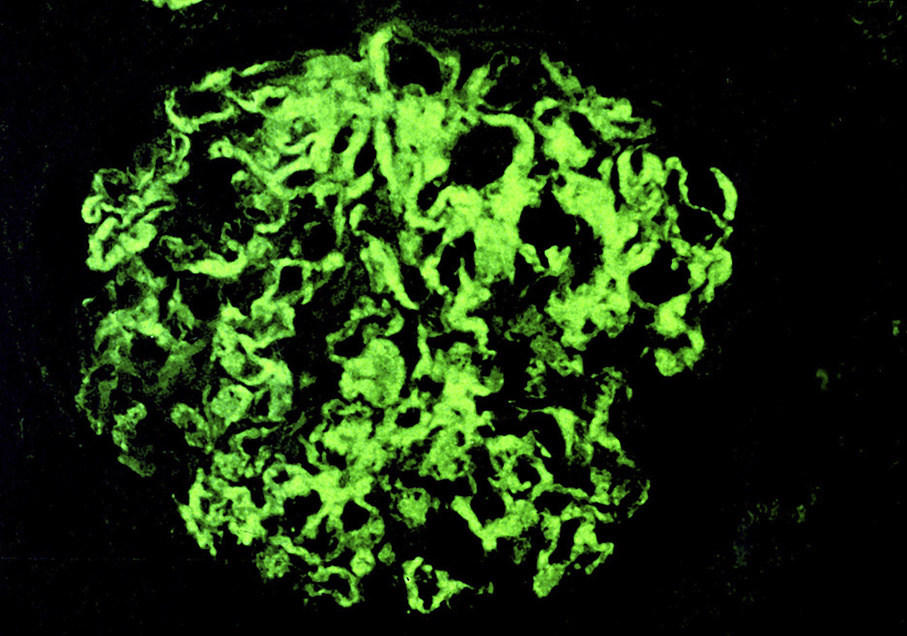
Immunofluorescence microscopy: Mesangial smudgy polyclonal immunoglobulin G (may be immunoglobulin G4 dominant) and C3, with smudgy, chunky capillary loop staining in proliferative cases, or granular capillary loop staining in membranous-pattern cases.
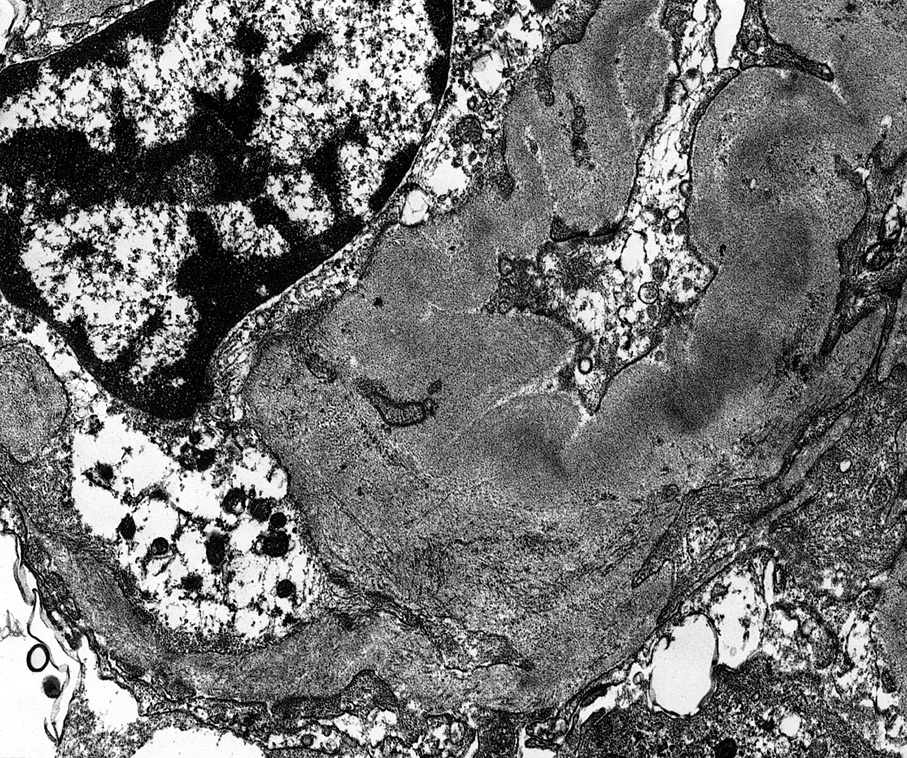
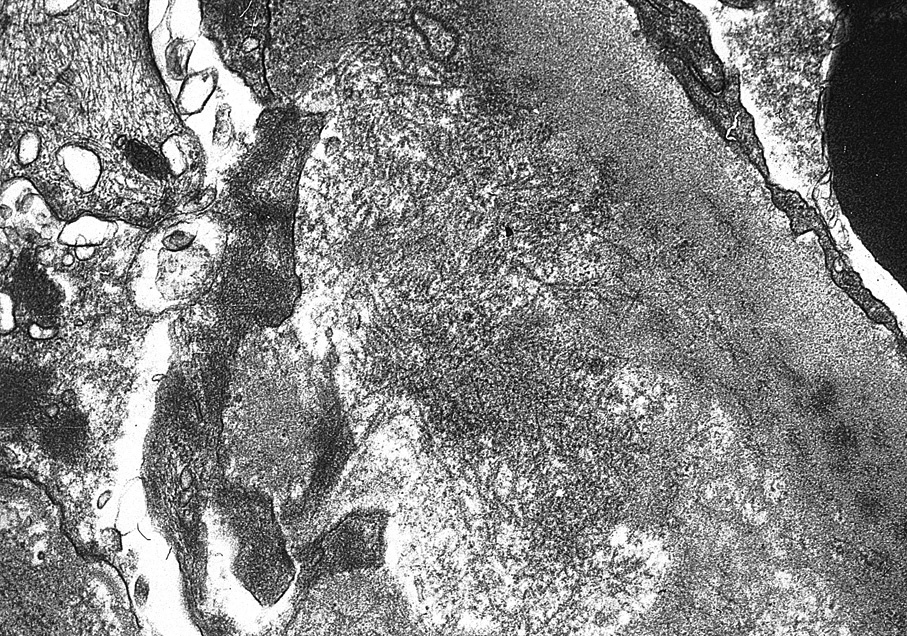
Electron microscopy: Randomly arranged nonbranching fibrillary deposits in the mesangium, and variably in the GBM, corresponding to the immunofluorescence pattern. Usual fibril diameter is 12-22 nm, contrasting with amyloid fibrils which range in thickness from 8-15 nm, but in most cases are between 10-12 nm.
The etiology of fibrillary glomerulonephritis has not been defined. This is a rare disease, accounting for 0.5-1% of native kidney biopsies, with no specific treatment. Crescents and more severe tubulointerstitial fibrosis have been associated with worse outcome.
Amyloid is distinguished from fibrillary glomerulonephritis by its Congo red positivity, smaller fibrils, and acellular mesangial expansion. Cryoglobulinemic glomerulonephritis is most often immunoglobulin M dominant with a clonal element, with microtubular or short, vague fibrillary substructure of deposits by electron microscopy. Immunotactoid glomerulopathy has monoclonal or oligoclonal deposits with larger, often microtubular deposits >30 nm diameter, in organized, parallel arrays. Fibronectin glomerulopathy shows short, vague fibrillary substructure revealed by electron microscopy, but is without immunofluorescence staining for immunoglobulins. Collagenofibrotic glomerulopathy also shows negative immunofluorescence, with banded type III collagen within the mesangium and in the subendothelial regions of capillary walls, but not permeating the GBM.