Microscopy Images
Immunotactoid glomerulopathy occurs in adults, on average at 60 years of age, and often presents with nephrotic proteinuria, reduced glomerular filtration rate, and hypocomplementemia in half of affected patients. Patients do not have cryoglobulins, but a circulating monoclonal paraprotein and/or lymphoplasmacytic malignancy is present in about two-thirds.
Prognosis depends on the outcome of the associated disease, with half of the affected patients achieving remission with therapy directed at the malignancy. This rarely leads to end-stage kidney disease. Recurrence in transplanted kidneys has been reported.
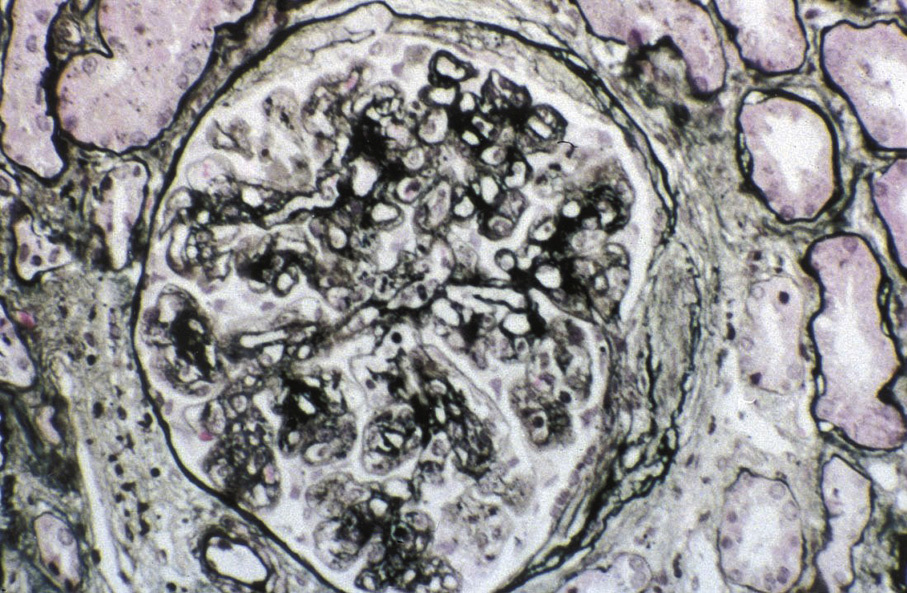
Light microscopy: Variable appearance, most commonly a membranoproliferative pattern or less frequently membranous pattern, and occasionally endocapillary proliferation.
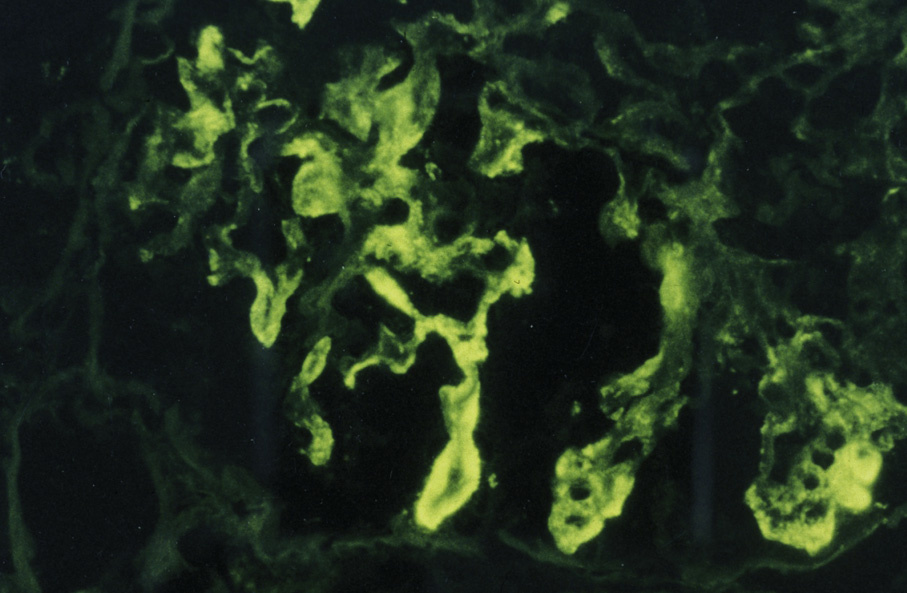
Immunofluorescence microscopy: Mesangial and chunky capillary wall immunoglobulin G, which is often clonal, and less C3, with a light chain restriction. Granular capillary loop staining is seen in cases with a membranous pattern.
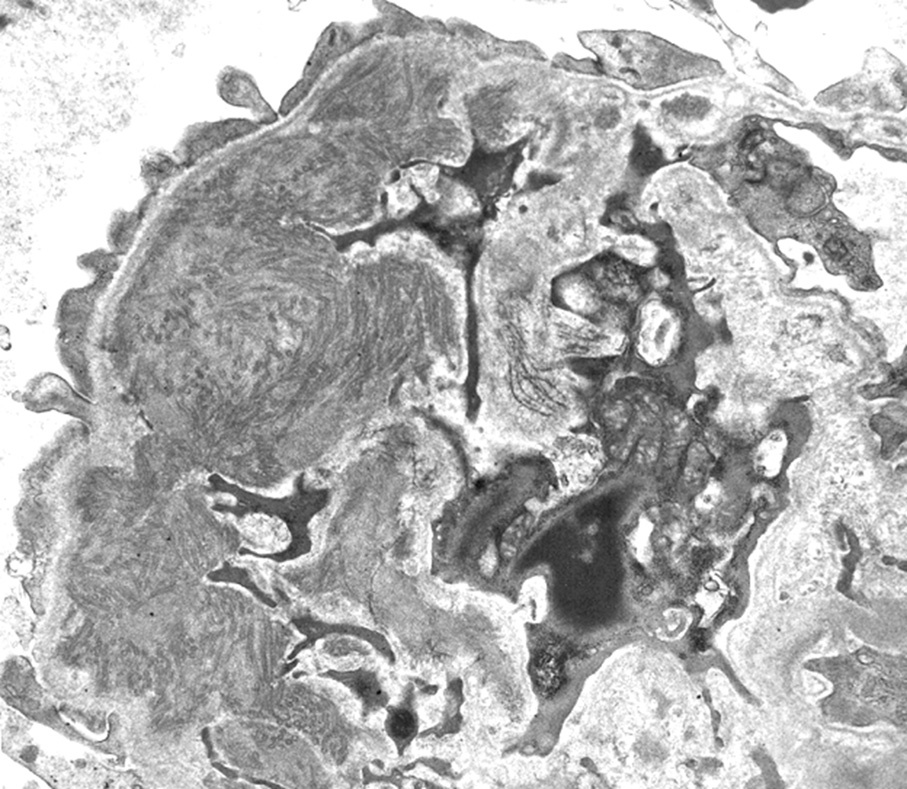
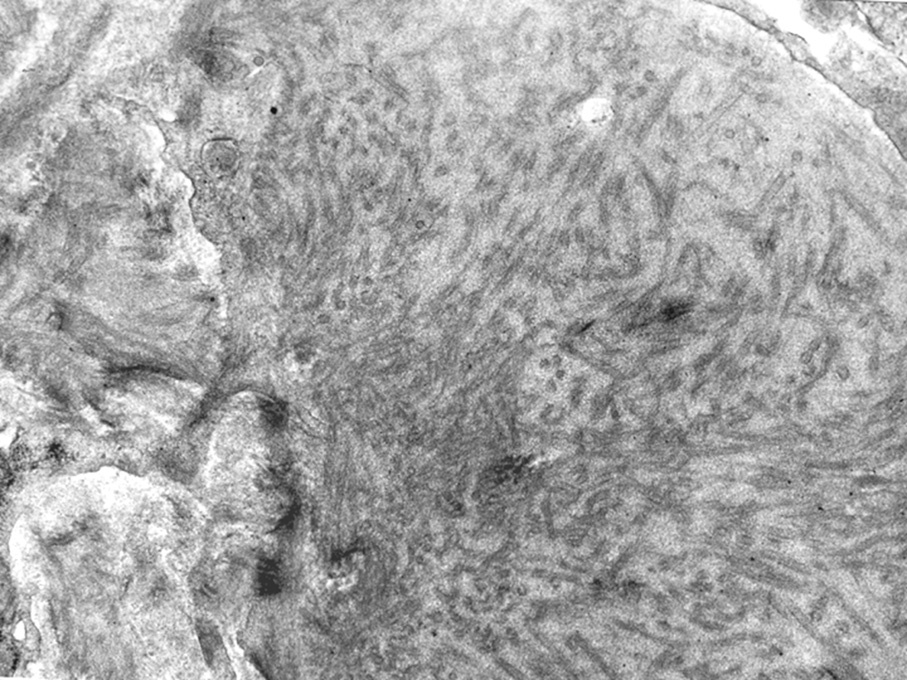
Electron microscopy: Microtubules, often in parallel arrays, with diameter typically >30 nm.
Immunotactoid glomerulopathy is associated with underlying lymphoplasmacytic disorders, and often has clonal deposits (ie, restricted to one light chain subclass) supporting a causal link of the deposits with the underlying malignancy.
Immunotactoid glomerulopathy is distinguished from fibrillary glomerulonephritis by the larger microtubular substructure revealed by electron microscopy, and the often clonal staining.
Cryoglobulinemic glomerulonephritis is most often immunoglobulin M dominant, can also be clonal, and has deposits with microtubular or short, vague fibrillary substructure revealed by electron microscopy.
Type I monoclonal cryoglobulin deposits may show an appearance indistinguishable from immunotactoid glomerulopathy, and the more common mixed cryoglobulinemic deposits also sometimes can show parallel arrays or microtubules. Some other entities with substructure of deposits revealed by electron microscopy do not show immunofluorescence positivity for immunoglobulins, such as fibronectin glomerulopathy or collagenofibrotic glomerulopathy.