Microscopy Images
Acute gouty nephropathy is caused by precipitation of uric acid crystals in tubules, usually collecting ducts. Patients with acute gouty nephropathy present with severe hyperuricemia and acute oliguric or anuric kidney failure. This often occurs secondary to tumor lysis syndrome or crush injury. Uric acid calculi may occur in acute gouty nephropathy in 15%-20% of patients. Chronic gouty nephropathy is related to deposition of monosodium urate crystals primarily in the medulla and is usually seen in patients with gout, chronic hyperuricemia, and hypertension.
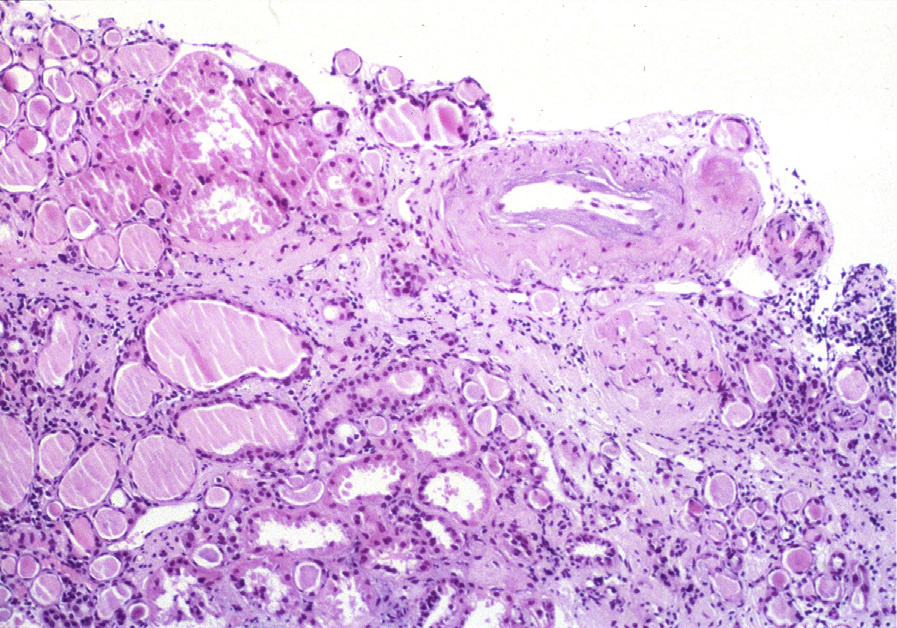
Light microscopy: Acute gouty nephropathy shows intraluminal clusters of urate crystals in collecting ducts with associated acute tubular injury. Tubulointerstitial inflammation is mild when present.
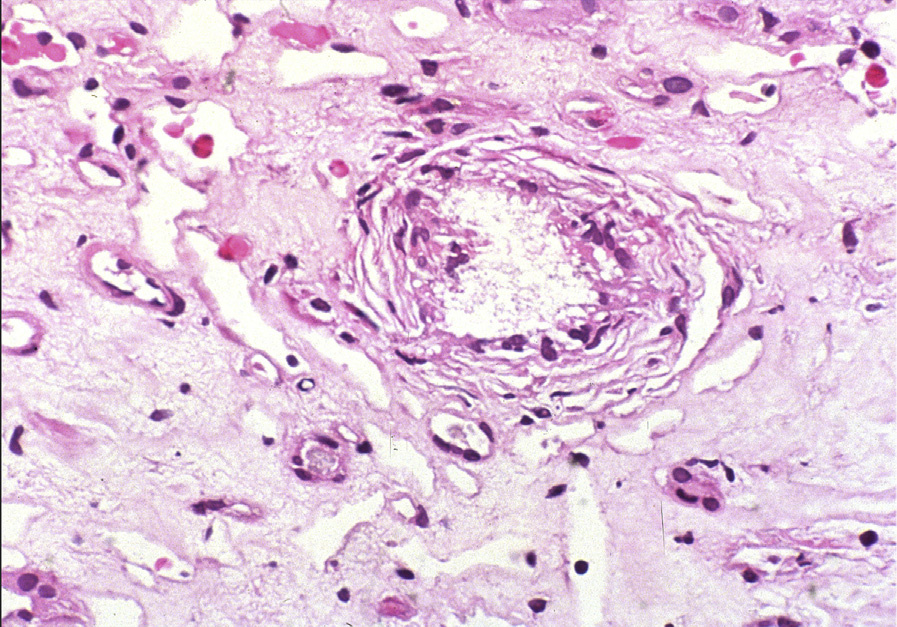
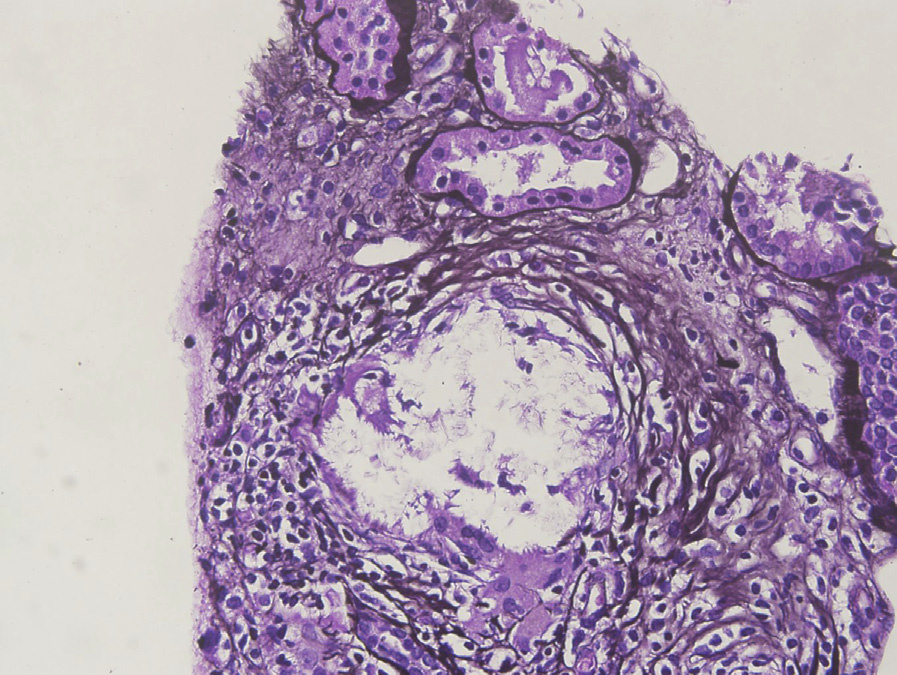
Needle-like birefringent crystals of monosodium urate can be seen in alcohol-fixed or frozen sections. These crystals are dissolved during processing of paraffin-embedded tissue and then appear as needle-like clefts. Chronic gouty nephropathy shows medullary intratubular and/or interstitial microtophi composed of central needle-shaped clefts with surrounding cellular reaction that includes syncytial giant cells, epithelioid macrophages, lymphocytes, and eosinophils. Tubulointerstitial fibrosis is variable. Glomerular changes can include increased mesangial matrix and double contours of glomerular basement membranes (GBMs).
Immunofluorescence microscopy: Noncontributory.
Electron microscopy: Collecting ducts show epithelial injury and cytoplasmic needle-like crystals.
The lamina rara interna is widened in cases with GBM double contours.
Uric acid is the final metabolic degradation product of purine. Uric acid is filtered, reabsorbed, secreted, and then reabsorbed again in the proximal tubule. Increased plasma uric acid occurs due to overproduction (10%-25% of cases) or decreased excretion (75%-90%). Overproduction is usually idiopathic (60%) or can occur with massive tissue destruction causing increased purine release, as with tumor lysis syndrome, crush injury, or intractable seizures. Overproduction may also be caused by hereditary enzyme deficiencies, as in X-linked hypoxanthine-guanine phosphoribosyltransferase deficiency (Lesch-Nyhan syndrome) and autosomal recessive glucose-6-phosphatase deficiency (glycogen storage disease type 1). Decreased excretion may be idiopathic, drug related (eg, thiazide diuretics, cyclosporine A), or due to chronic heavy metal toxicity, metabolic disorders including Bartter syndrome, endocrine disorders (hypothyroidism, hyperparathyroidism), or uromodulin storage disease.
Acute tubular injury can occur secondary to other crystalline deposits.
Indinavir and light chain tubulopathy involve proximal tubules, and the latter also shows monoclonal crystals by immunofluorescence. In contrast, gouty nephropathy involves collecting ducts in the medulla. Tophi are distinguished from other causes of granulomatous inflammation by the central, feathery, needle-shaped crystals, in contrast to cholesterol granulomas (with intratubular lancet-shaped crystals) or sarcoidosis (which does not have crystals and demonstrates multiple, confluent granulomas).