Microscopy Images
Indinavir toxicity is a classic example of the druginduced nephrotoxicity seen with several antiviral drugs. Patients may be of any age, and present with AKI. Other antiviral drugs may cause similar AKI (eg, acyclovir, foscarnet). Up to 67% of indinavir-treated patients have asymptomatic crystalluria, with symptoms in 8% and nephrolithiasis in 3%. Birefringent indinavir crystals may be seen in the urine, occasionally with sterile pyuria.
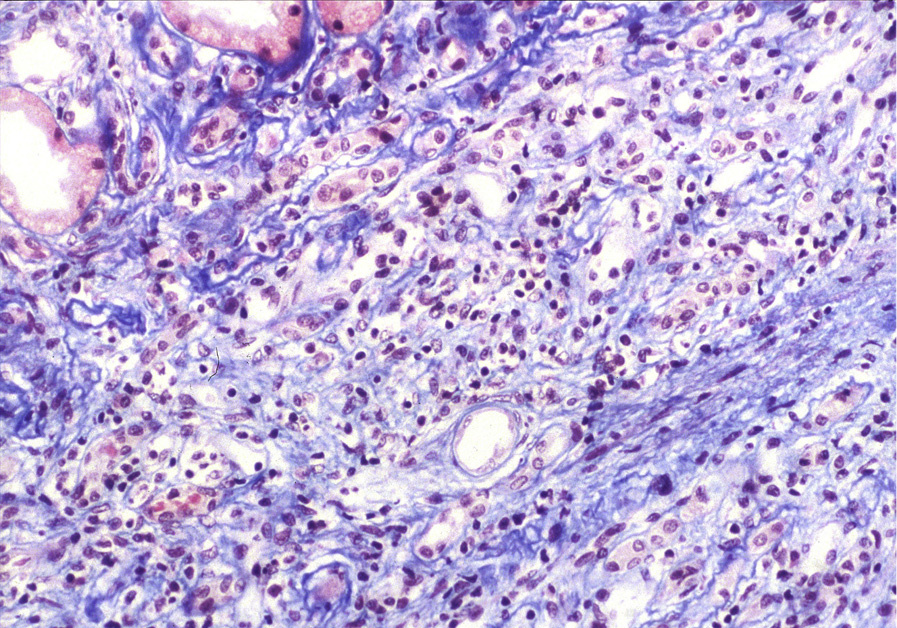
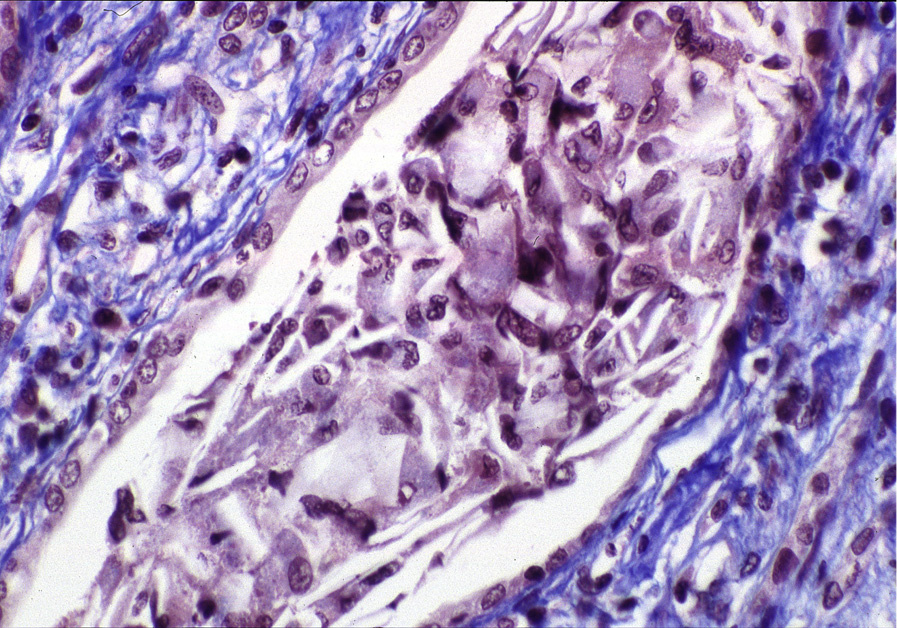
Light microscopy: There is acute tubular injury with clear rectangular crystals in tubular lumina with surrounding intratubular mononuclear cell reaction, occasionally extending to the surrounding interstitium.
Glomeruli are unremarkable.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: No specific findings.
Indinavir is an antiviral protease inhibitor that is excreted in the urine, and is insoluble at normal physiologic urine pH. Higher doses, higher ambient temperatures, pre-existing kidney disease, low body weight, lack of adequate hydration, coinfection with hepatitis C virus, and coexisting therapy with trimethoprim-sulfamethoxazole increase the risk of crystal formation. Crystals precipitate in the tubules, causing acute tubular injury with consequent AKI.
Patients may also have nephrolithiasis.
Other protease inhibitors may cause similar crystalluria. Cholesterol crystals, which may be present within tubules in patients with marked proteinuria and lipiduria, have tapered needle-like edges, and may on occasion cause so-called cholesterol granulomas with surrounding giant cell reaction.