Microscopy Images
Kidney disease is a common manifestation in HIV-infected patients, with albuminuria reported in 10%-15%. The vast majority, around 90%, of HIVAN patients are of African descent. Patients may present at any age. The spectrum of disease in HIV-infected patients varies, from HIVAN, which is manifest by collapsing glomerulopathy, to other forms of FSGS, minimal change disease, thrombotic microangiopathy, and lupus-like HIV-immune complex kidney disease (HIVICK). Kidneys are often enlarged in HIVAN patients. Patients with HIVAN manifest nephrotic syndrome, often have increased serum creatinine at presentation, and show rapid progression, with about half reaching ESRD after 3 years. The prevalence of HIVAN among HIV-infected individuals has decreased dramatically since the advent of combination antiretroviral therapy (cART) as standard of care for these patients.
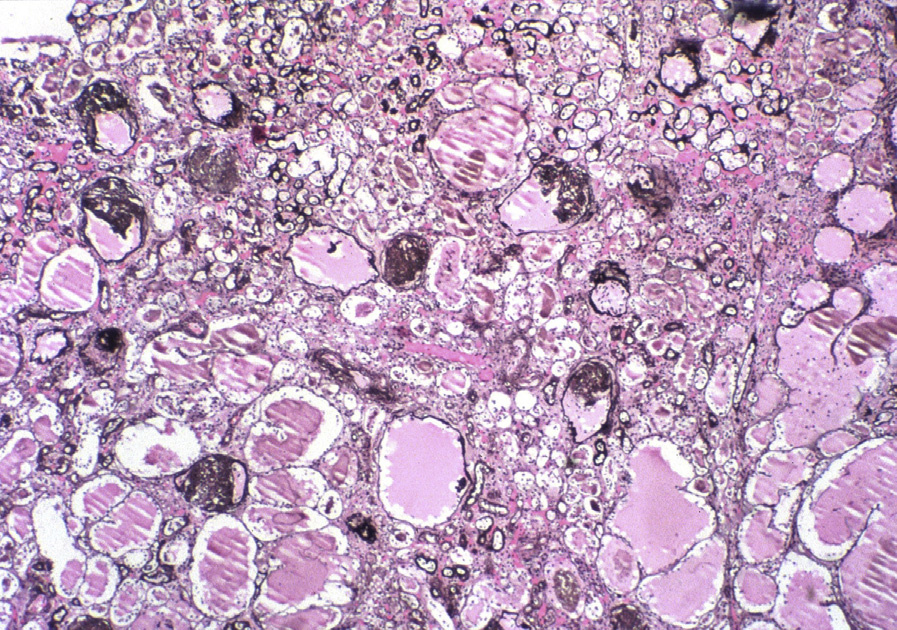
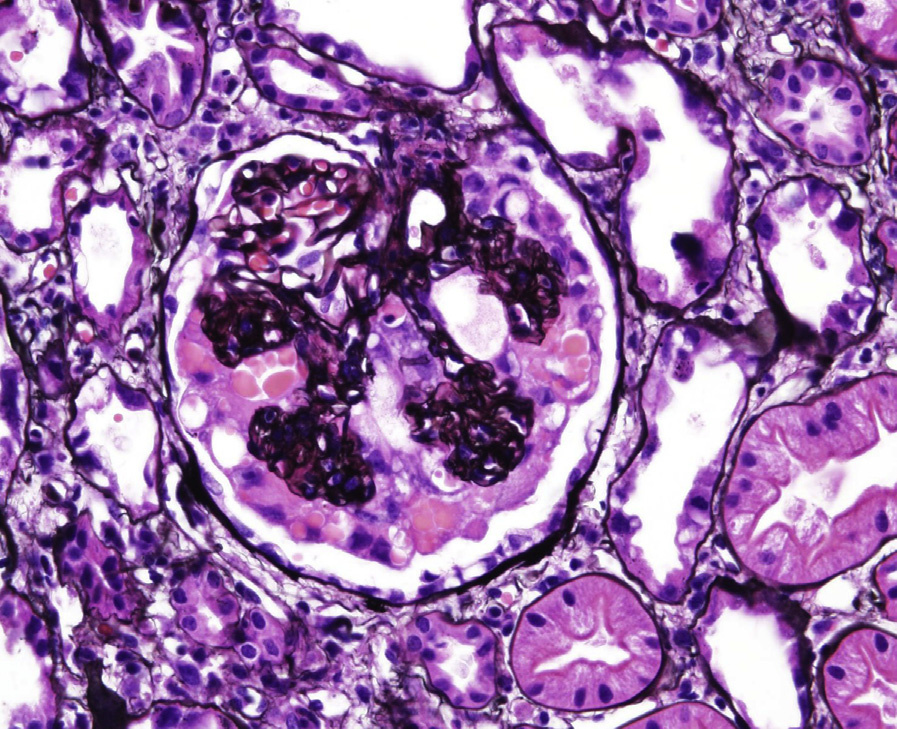
Light microscopy: Segmental or global glomerular tuft collapse with overlying visceral epithelial hyperplasia and hypertrophy is seen. Hypertrophied visceral epithelial cells have frequent protein droplets.
There is accompanying microcystic tubular dilatation and active tubulointerstitial nephritis with a predominantly lymphocytic infiltrate, often with tubulitis and edema.
Immunofluorescence microscopy: No or limited immune deposits (nonspecific IgM and C3 staining in collapsed segments) are identified. Protein droplets in visceral epithelial cells may stain for immunoglobulins and albumin.
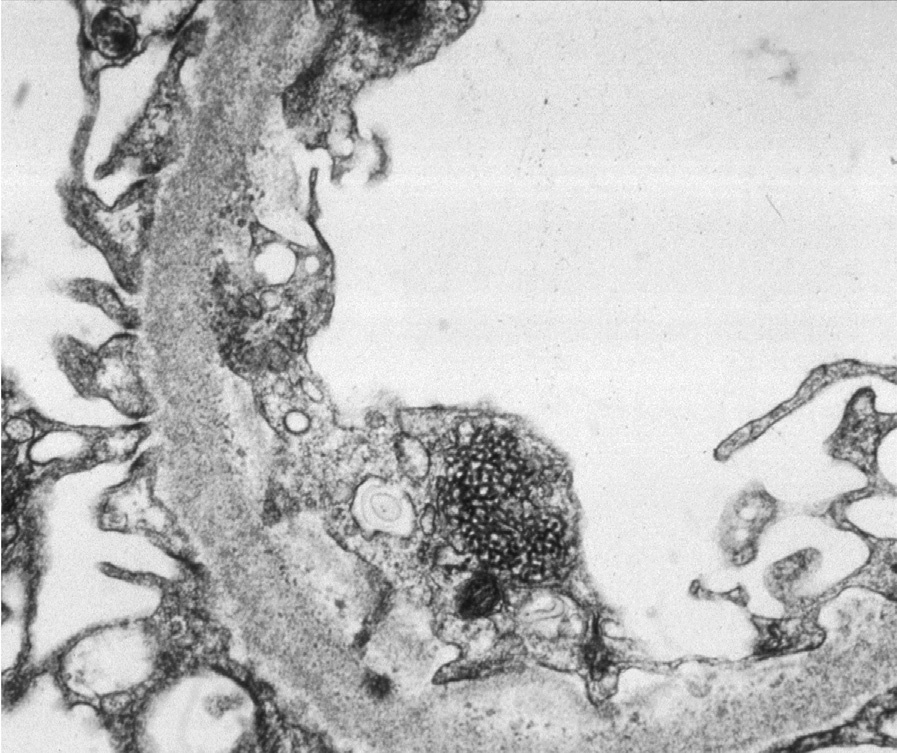
Electron microscopy: Glomerular basement membranes are wrinkled and collapsed. Overlying visceral epithelial cells show hypertrophy and hyperplasia, with frequent vacuoles and protein droplets. There is extensive foot process effacement and no or limited mesangial deposits. Tubuloreticular aggregates are present in endothelial cells, in contrast to idiopathic collapsing glomerulopathy, in which such aggregates are typically absent. Tubuloreticular aggregates may be rare or even absent in patients with low viral loads who are receiving cART.
HIVAN is due to HIV infection, with experimental evidence supporting a scenario that direct infection of kidney epithelial cells is sufficient for disease. Patients with a risk allele variant of APOL1, common in African Americans, have a markedly increased incidence of HIVAN.
Crescentic glomerulonephritis has parietal epithelial proliferation, but generally does not have protein reabsorption droplets in the epithelial cells. Crescents are also often accompanied by segmental necrosis and glomerular basement membrane breaks with fibrinous exudates, features that distinguish them from collapsing lesions.
Collapsing glomerulopathy can be related to other infections (eg, parvovirus), drugs (eg, bisphosphonates and calcineurin inhibitors), severe vascular disease (eg, thrombotic microangiopathy and cocaine use), and autoimmune disease (eg, systemic lupus erythematosus), or may be idiopathic. A clinical history of HIV infection and the presence of tubuloreticular aggregates indicate HIVAN as the etiology of the collapsing lesions.