Microscopy Images
Amyloidosis is a systemic disease caused by amyloid deposition, which may be due to a monoclonal protein, hereditary disorders, or other conditions (see also AL Amyloidosis). The type is diagnosed by immunofluorescence (IF), immunohistochemistry (IHC), and/or mass spectrometry (MS). Hereditary amyloids are autosomal dominant, and are caused by mutation in one of various proteins, most commonly transthyretin (A TTR) but also apolipoprotein AI, AII, or AIV (A ApoAI/II/IV); gelsolin (A Gel), lysozyme (A Lys), cystatin C (A Cys), and fibrinogen Aa-chain (A Fib). Patients present at older age with symptoms dependent upon organ involvement, commonly including heart, GI tract, nerves, and kidney (typically manifesting as nephrotic proteinuria). No specific treatment is available, but liver transplantation may remove the major source of amyloid in some (eg, A Fib).
Secondary amyloid may involve a variety of proteins. Serum amyloid A protein (SAA), an acute phase reactant, increases with chronic inflammation, and may occur at any age in patients with underlying conditions such as rheumatoid arthritis, familial Mediterranean fever, or chronic infections. Dialysis-associated amyloid is due to β2-microglobulin.
Leukocyte chemoattractant factor 2 (LECT2) amyloid is of unknown etiology. These patients are older and mostly Mexican American, with sex balance.
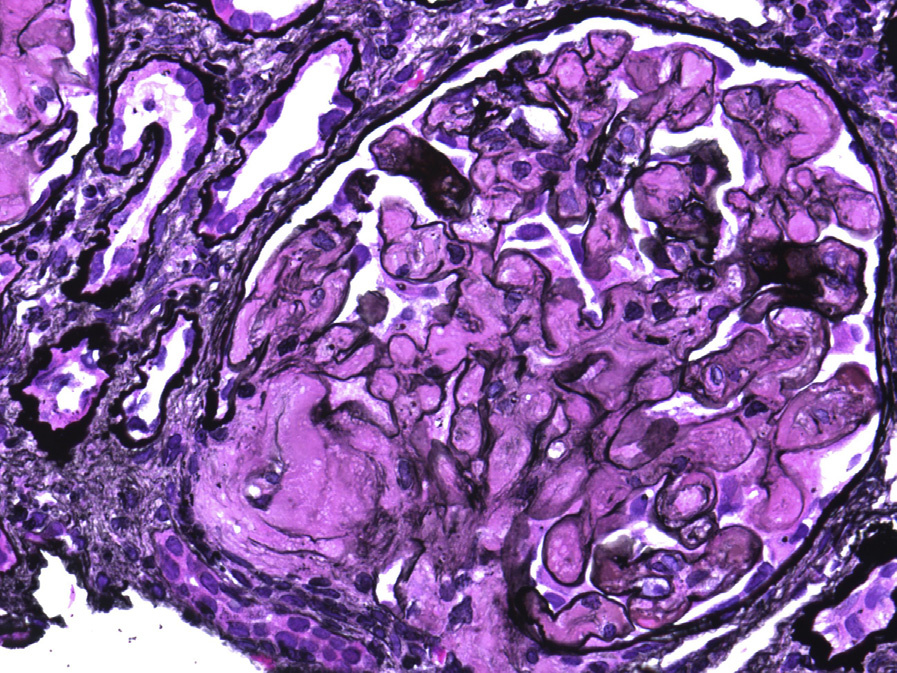
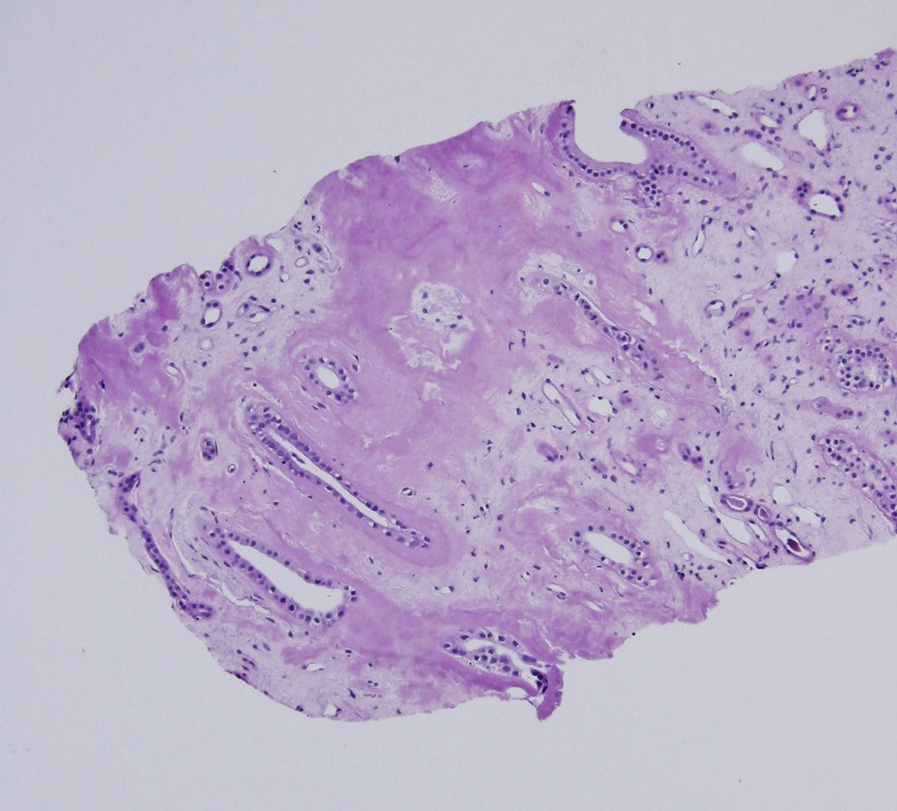
Light microscopy: Amyloid deposits involve the mesangium as acellular, amorphous, silver-negative, pale pink, cotton candy–like material.
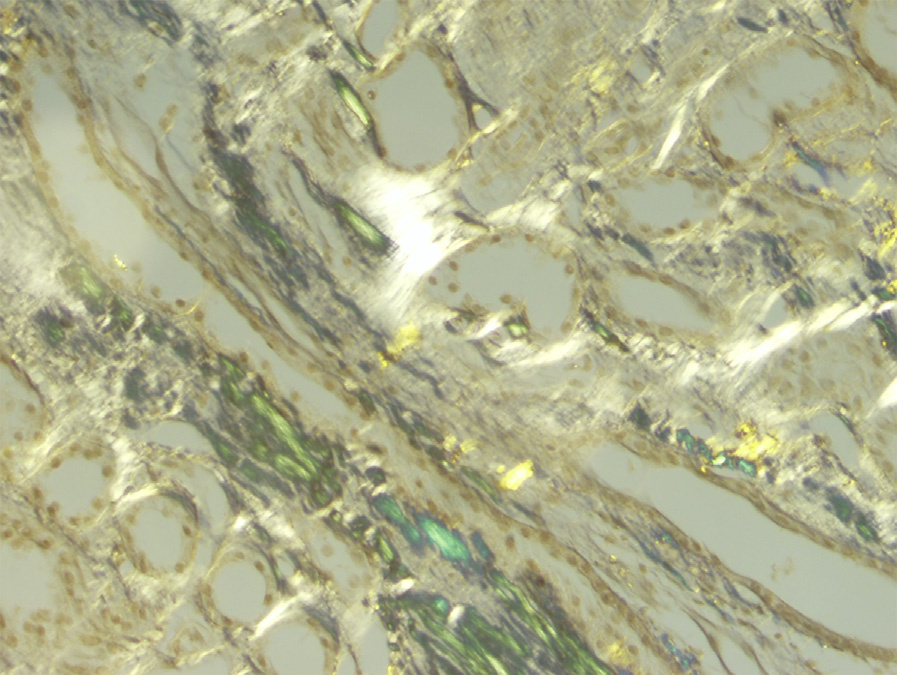
Amyloid involving the GBMs results in segmental, long, feathery, silver-positive spikes. Arterioles and arteries often also show amyloid deposits. Interstitial and tubular basement membrane amyloids have a similar pale pink acellular appearance. Diagnosis is by Congo red positivity, with apple-green birefringence under polarized light. LECT2 and ApoA amyloids often show prominent interstitial involvement, while A Fib dominantly involves glomeruli.
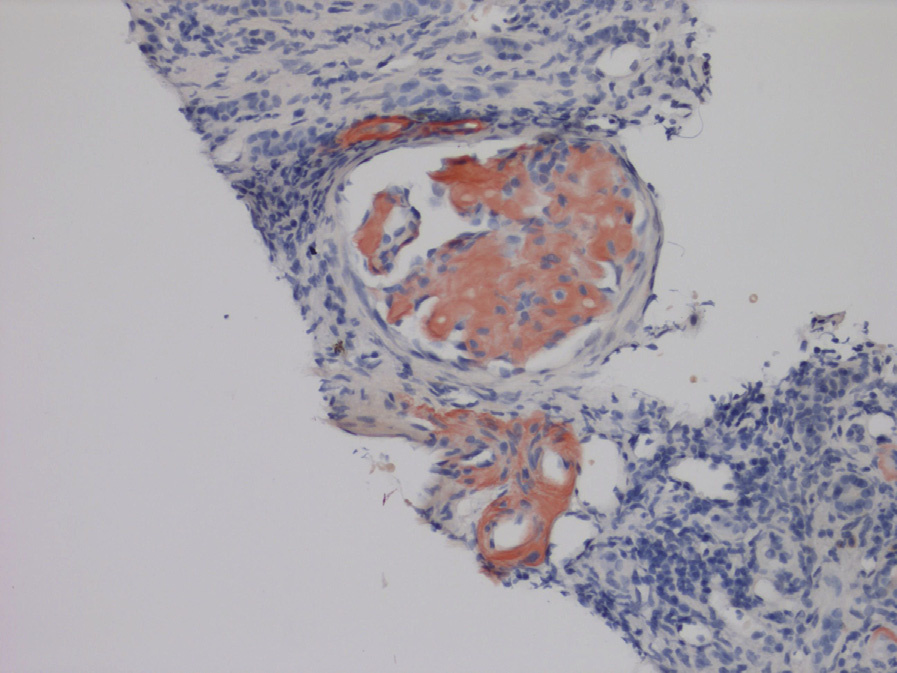
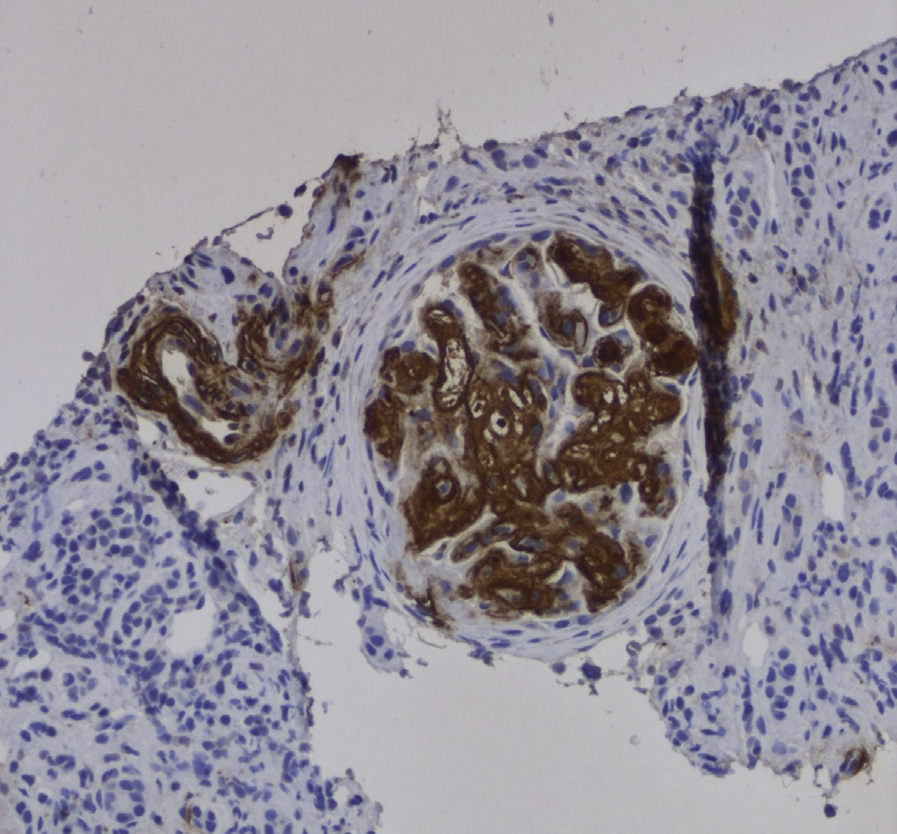
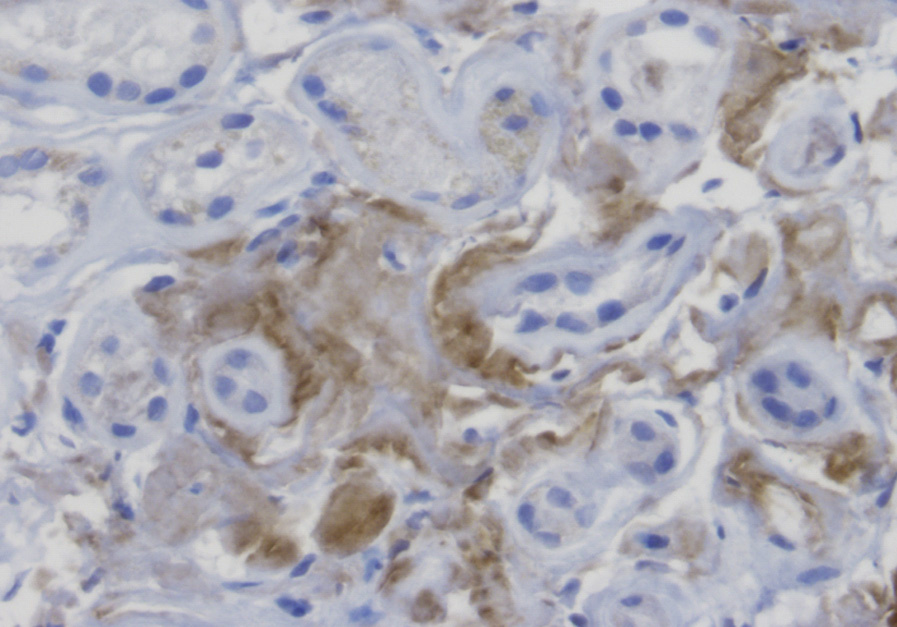
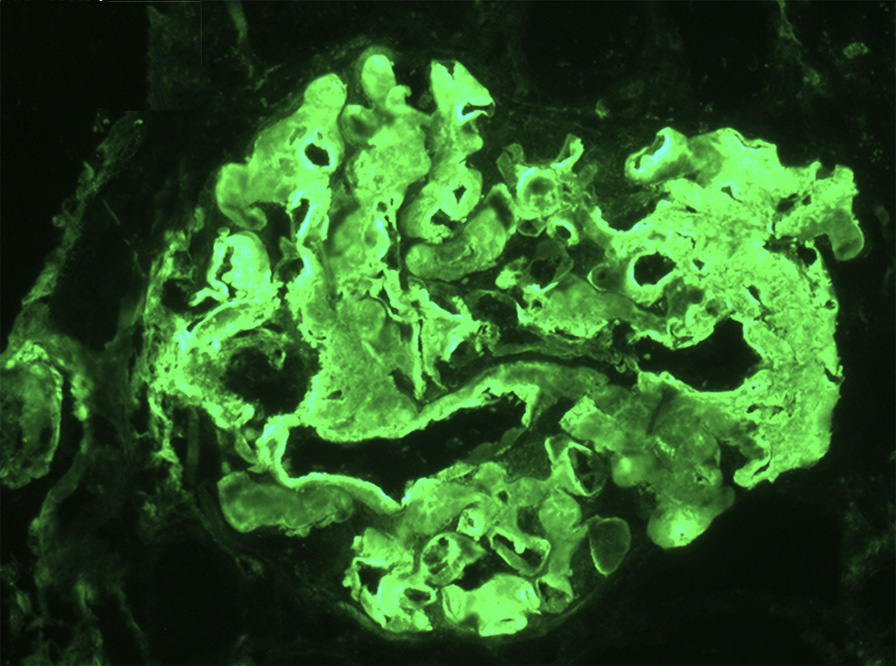
IF/IHC microscopy: Standard IF is negative or nonspecific. Specific IHC and/or laser microdissection–MS can type the amyloid in such cases.
Electron microscopy (EM): Amyloid fibrils are extracellular, straight, randomly arranged, and measure 9-11 nm in diameter. These can be found in the mesangium and GBMs, causing mesangial expansion and irregular thickening of the basement membranes, with typical projections extending towards podocytes with extensive foot process effacement.
Extraglomerular deposits in vessel walls, tubular basement membranes, or interstitium may be present.
Amyloids are due to proteins that form a beta-pleated sheet, which accounts for the Congo red intercalation and apple-green birefringence. Beta pleats resist proteolysis, and progressive amyloid deposition results in organ dysfunction. Hereditary amyloid is due to a protein mutation. Other forms of amyloid include those related to chronic inflammatory conditions (SAA), β2-microglobulin in dialysis patients, and LECT2.
These forms of amyloid may be distinguished from other causes of mesangial expansion by negative IF, Congo red staining, and fibrils by EM. Distinction from AL amyloid is made by absence of light chain clonal staining. Fibrillary GN is Congo red negative, with polyclonal IgG, proliferative appearance, and thicker fibrils(10-30nm);diabetic nephropathy shows no fibrillary deposits; other monoclonal immunoglobulin deposition diseases are Congo red negative, with absence of amyloid fibrils on EM. Other causes of MPGN pattern show disease-specific IF and EM appearances.