Microscopy Images
Immunoglobulin A (IgA)-dominant infection-related glomerulonephritis is a morphologic variant of acute infection-related glomerulonephritis that typically occurs in association with staphylococcal infection. It is most common in older patients and those with diabetes, and rare in children. Patients typically present with acute kidney injury, proteinuria, and hematuria. Hypocomplementemia is present in the vast majority of the patients. The prognosis is poor, with less than 20% of patients fully recovering kidney function, most likely owing to age-related underlying kidney changes and comorbidities, including diabetic kidney disease. The most common site of infection is skin, including cellulitis, surgical wound infection, skin abscesses, and intravenous line infection. The most common infectious agents are Staphylococcus, including methicillin-resistant Staphylococcus aureus (MRSA).
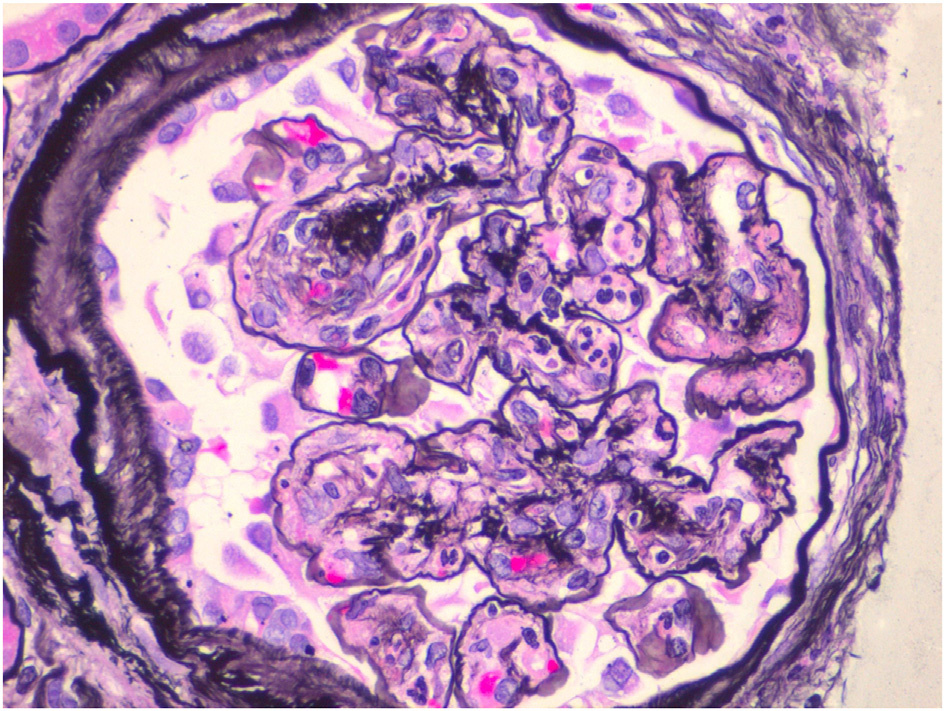
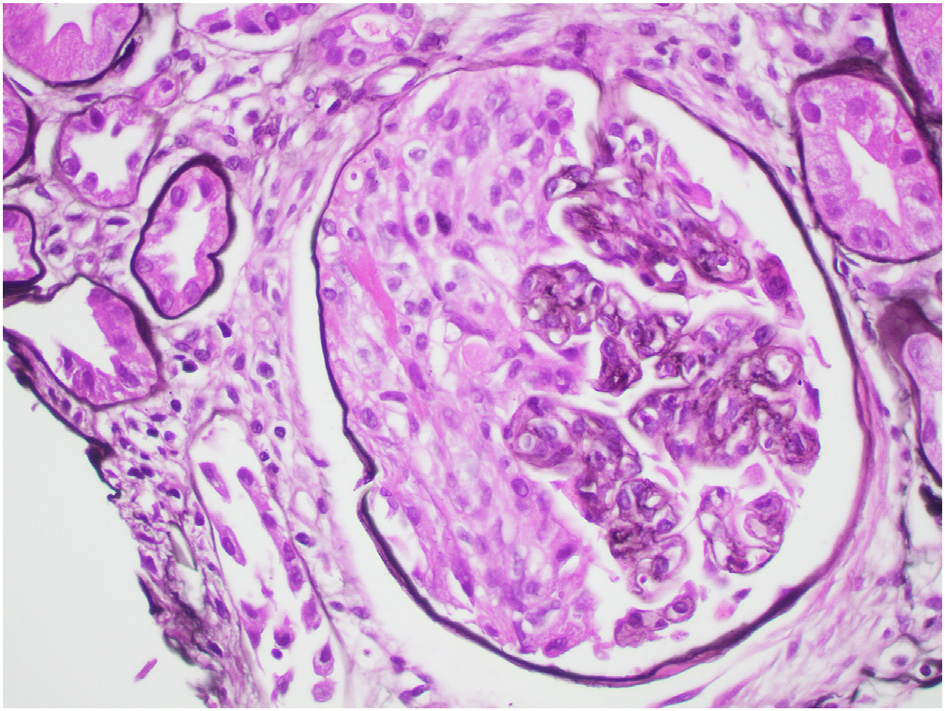
Light microscopy: Glomeruli show segmental to global endocapillary hypercellularity with frequent neutrophils.
Crescents may be present. Underlying changes of diabetic kidney disease may be present, including nodular glomerulosclerosis and arteriolar hyalinosis.
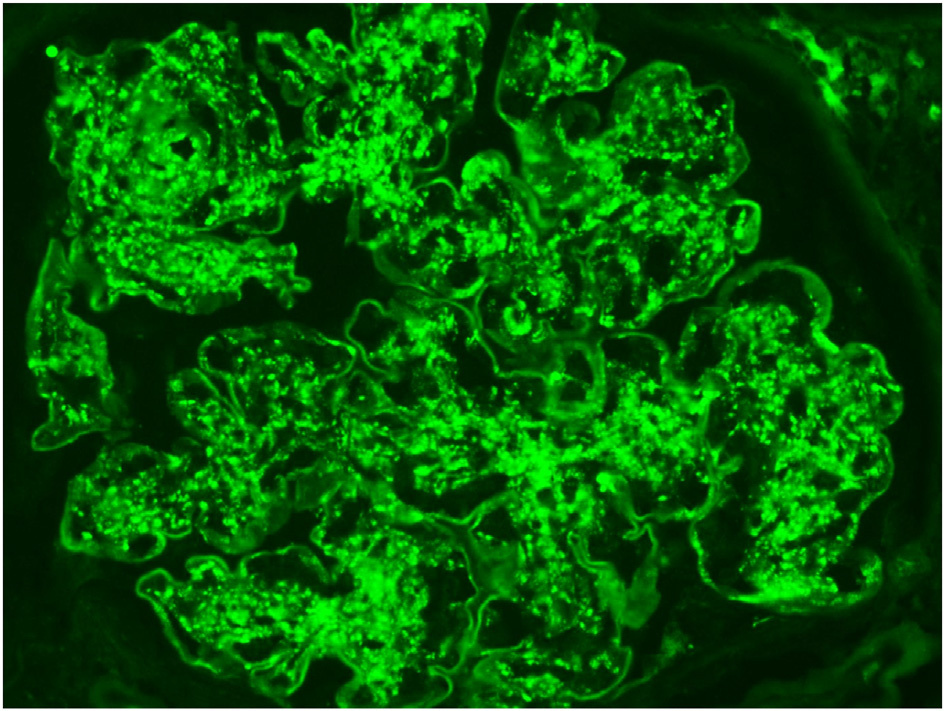
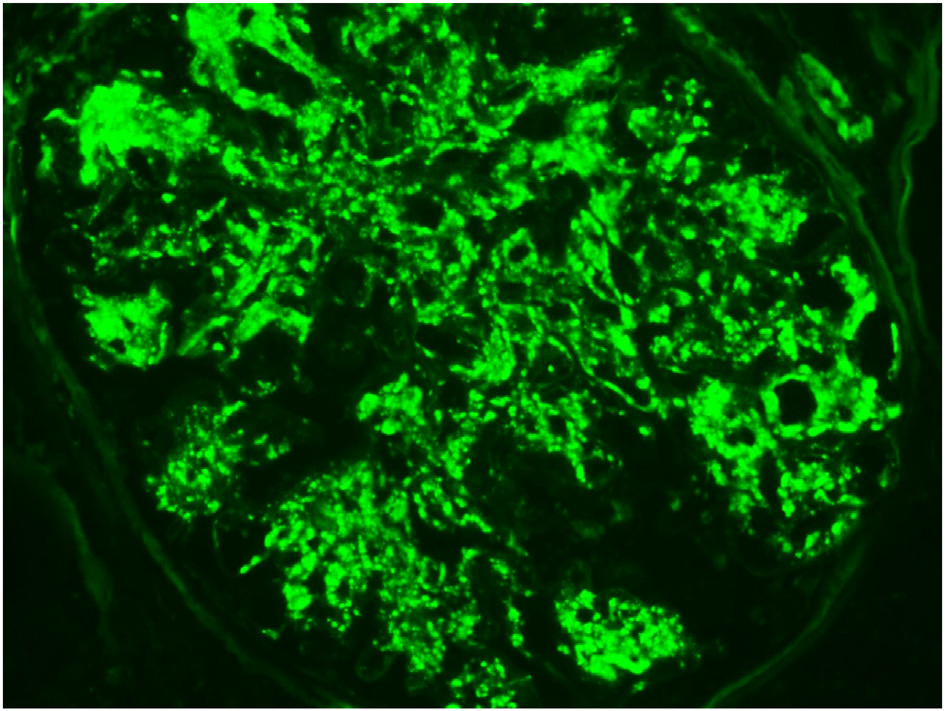
Immunofluorescence microscopy: Glomeruli show chunky, irregular mesangial and capillary wall polyclonal IgA with lesser staining for IgG and prominent C3. The deposits often show a garland or starry-sky appearance as in typical poststreptococcal-related glomerulonephritis. Unlike IgA nephropathy, λ light chain is not typically dominant.
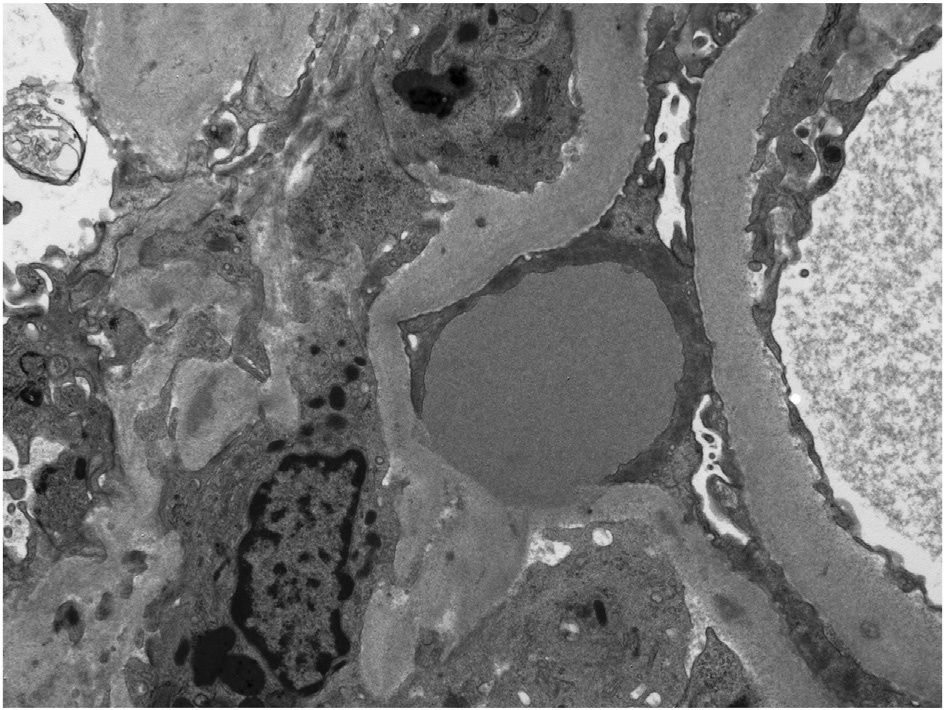
Electron microscopy: Glomeruli show endocapillary hypercellularity, frequent intracapillary neutrophils, occasional mesangial and small subendothelial deposits, and hump-type large subepithelial deposits without surrounding glomerular basement membrane reaction. In more chronic phases, humptype deposits may be sparse, located only in the hinge region.
Although the pathogenesis of IgA nephropathy is linked to presence of galactose-deficient IgA1, the pathogenic mechanism of the selective IgA deposition in IgA-dominant infection-related glomerulonephritis is not well understood but likely involves specific host-pathogen interaction. Immune complexes may be circulating or the bacterial-derived antigen can bind within the glomerulus, with antibody and complement activation occurring in situ. Increased serum IgA levels have been reported in some, suggesting activation of selective IgA immune response. Polyclonal increases of serum IgA and IgG, high levels of circulating IgA and IgG immune complexes, and massive T-cell activation are hypothesized to play a role in this entity. Staphylococcal enterotoxin has been proposed as a causative agent in this entity following MRSA infection.
Superantigens (enterotoxin) stimulate resting T cells to proliferate, causing a massive activation of T cells and a subsequent release of T cell–derived lymphokines (eg, interleukin 1, 2, or 6) and cytokines (eg, tumor necrosis factor α or interferon γ). More than 50% of patients with IgA-dominant infection-related glomerulonephritis have diabetes. Therefore, it is possible that the diabetic milieu plays a role in the mounting of an IgA-dominant immune response to the infection.
IgA-dominant infection-related glomerulonephritis should be distinguished from IgA nephropathy and IgA vasculitis (Henoch-Schönlein purpura nephritis). Clinical and histopathologic features that suggest IgA-dominant infection-related glomerulonephritis include initial presentation in elderly patients, acute kidney injury at presentation, staphylococcal infection, low serum complement, diffuse endocapillary hypercellularity with prominent neutrophil infiltration, stronger staining for C3 than IgA and lack of λ light chain predominance on immunofluorescence, and the presence of hump-type subepithelial deposits on electron microscopy. Some studies suggest that weak or negative staining for galactose-deficient IgA1 may favor IgA-dominant infection-related glomerulonephritis over IgA nephropathy, but this staining is not currently used in clinical practice and additional studies are needed to confirm this notion.