Microscopy Images
Postinfectious glomerulonephritis (GN) presents as acute nephritic syndrome with low complement C3 in serum, commonly following streptococcal throat or skin infection. Other infections may also give rise to postinfectious GN. Postinfectious GN most commonly occurs in children or young adults. The prognosis is excellent in children when the underlying infection resolves. Older adults, often diabetic or immunocompromised, may also develop postinfectious GN, more often from visceral sites of infection, and have a poor prognosis with frequent progression to end-stage kidney disease.
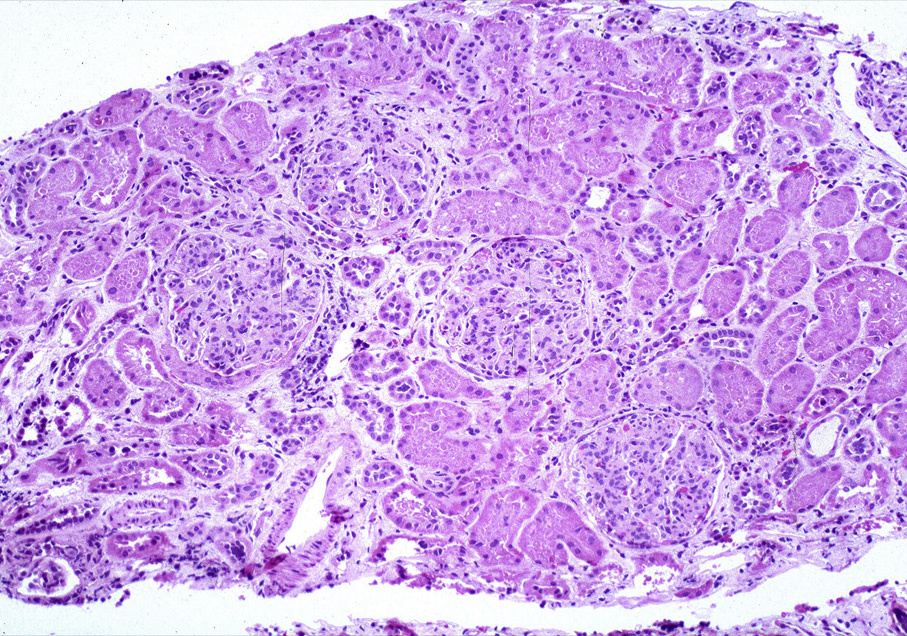
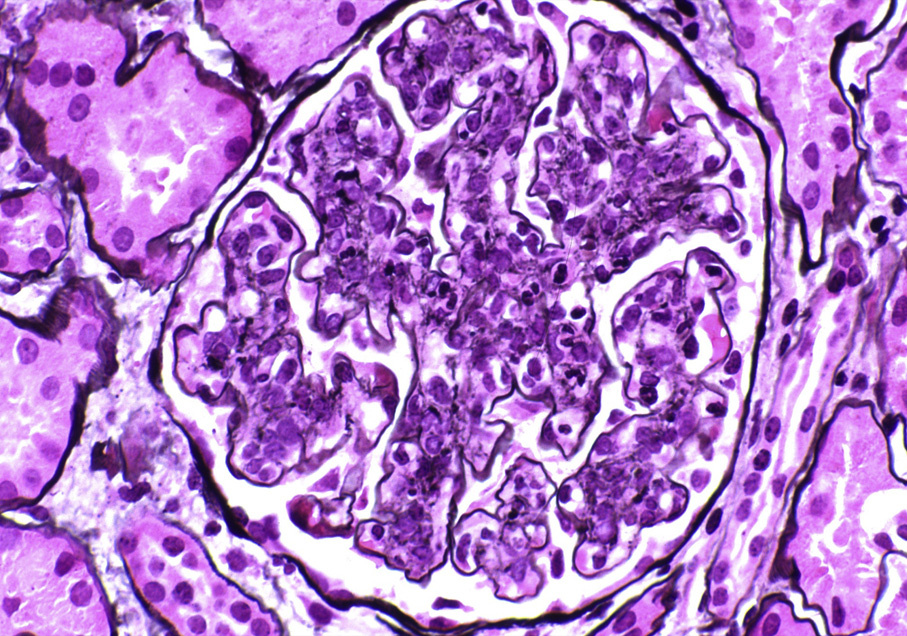
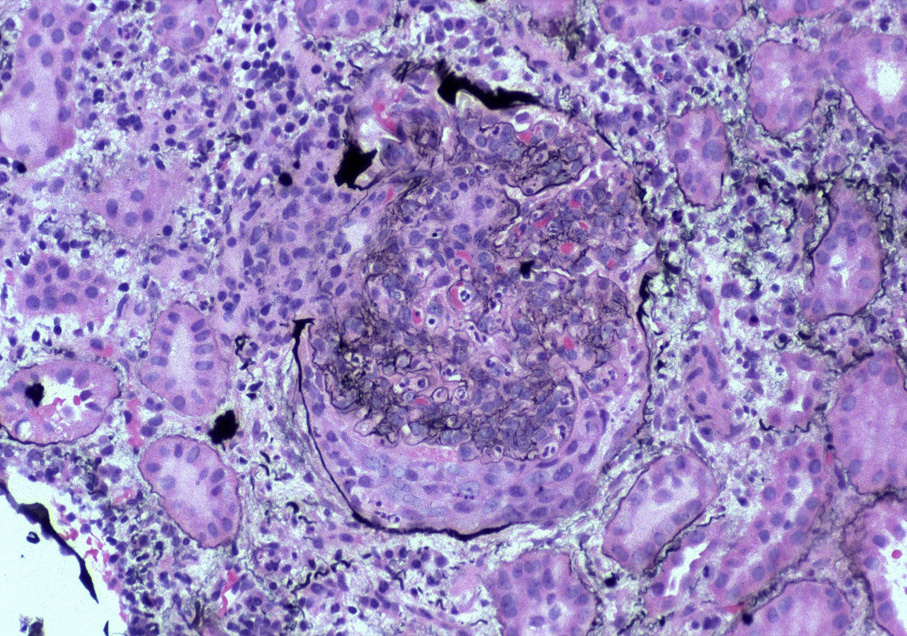
Light microscopy: Segmental or global endocapillary hypercellularity, with frequent neutrophils. Crescents may be present.
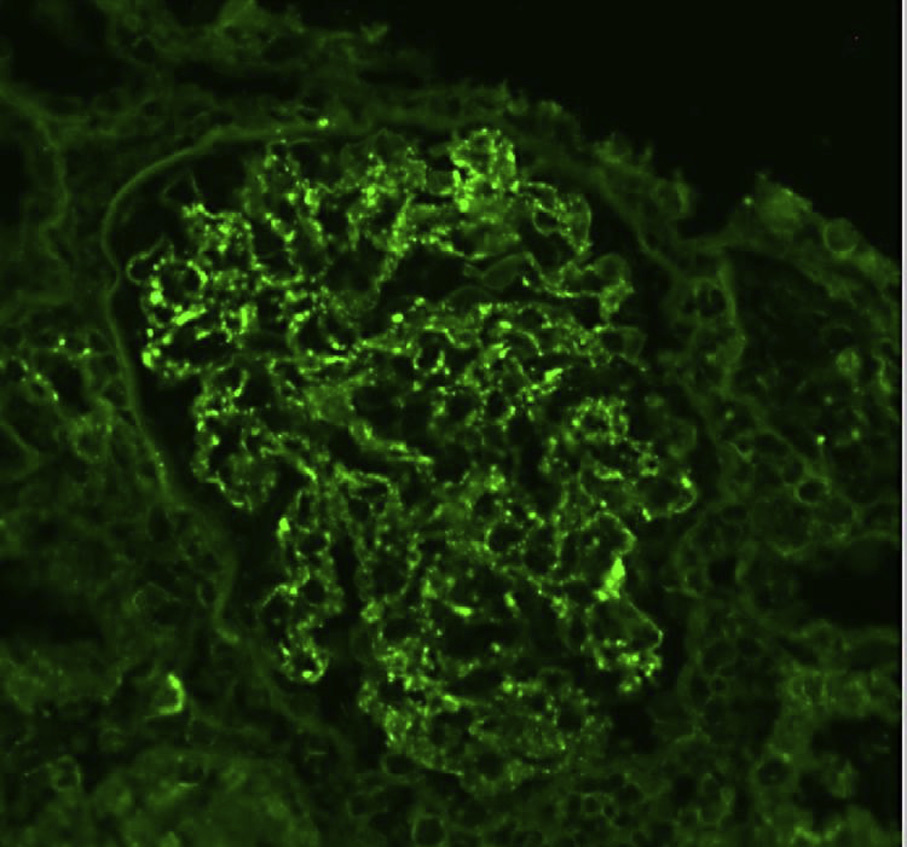
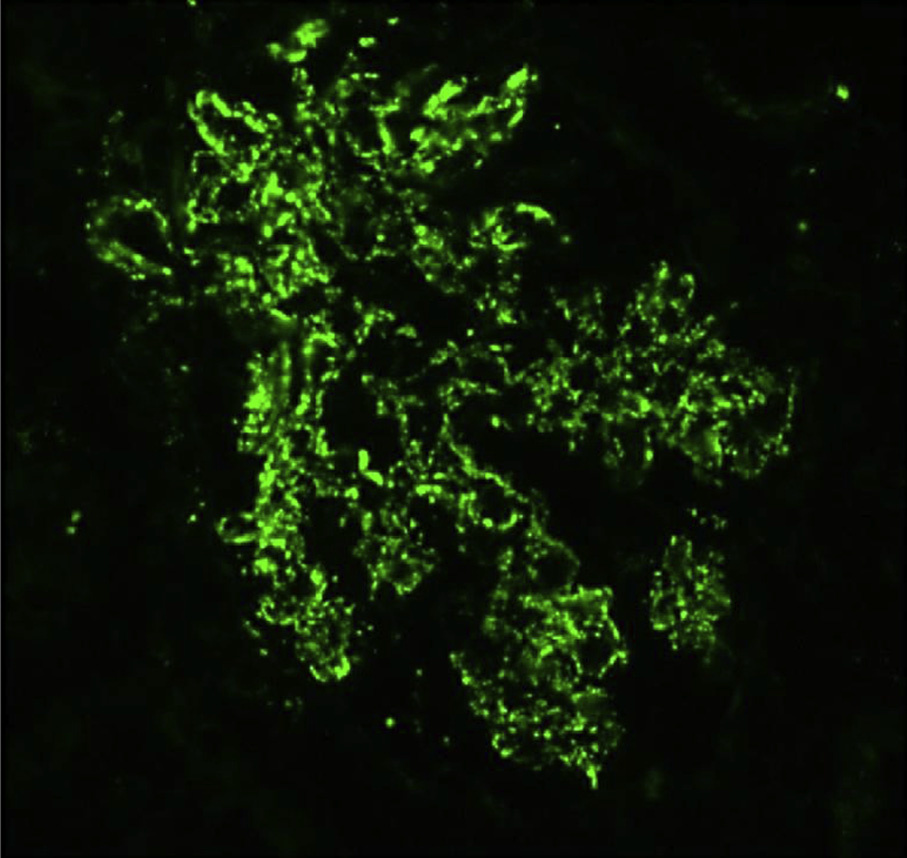
Immunofluorescence microscopy: Typically, polyclonal IgG and prominent C3 in chunky, irregular mesangial and capillary wall pattern (“garland” or “starry sky” appearance). Immunoglobulin A may be the dominant immunoglobulin deposited, particularly in older and diabetic patients.
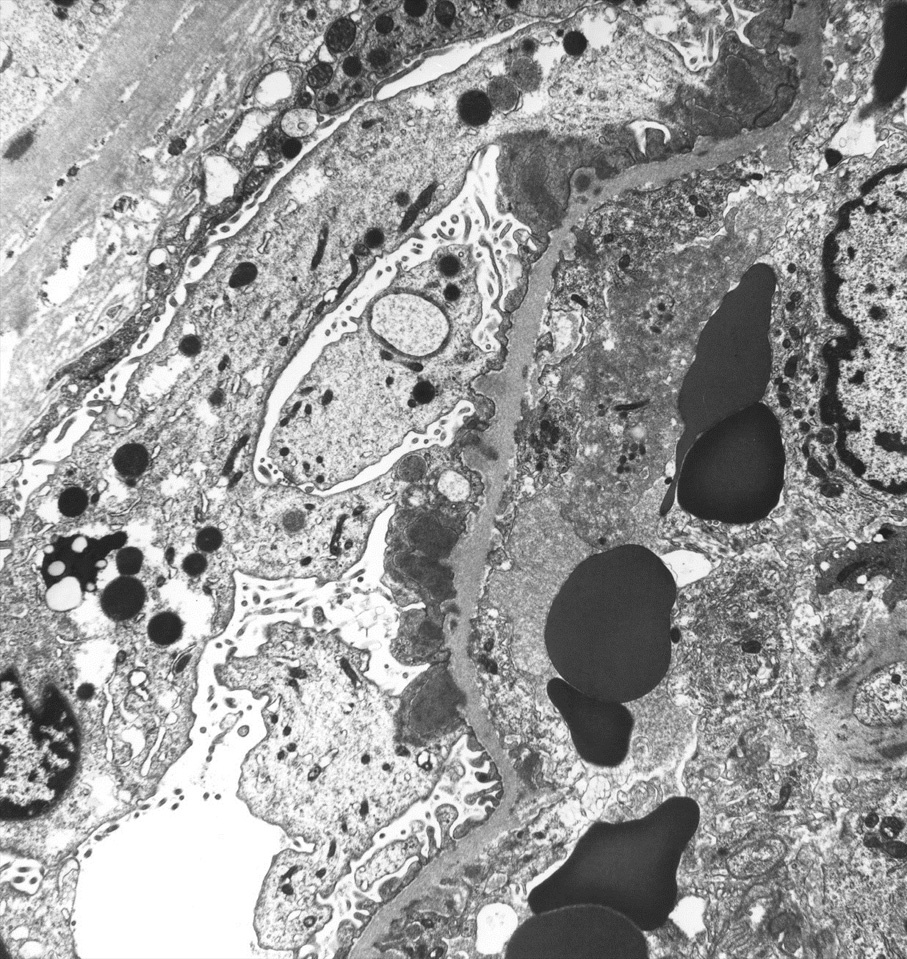
Electron microscopy: Endocapillary hypercellularity, frequent neutrophils, occasional mesangial and small subendothelial deposits, and hump-type large subepithelial deposits without surrounding glomerular basement membrane reaction.
Antigens of infectious agents activate the alternative complement pathway. Immune complexes may be circulating, or antigens can bind within the glomerulus with antibody and complement activation occurring in situ. Streptococcal pyrogenic exotoxin B has been proposed as a causative antigen in postinfectious GN following group A streptococcal infection.
Subepithelial humps are highly suggestive of postinfectious GN, but may also be seen in C3 GN. Other immune complex diseases may have endocapillary hypercellularity shown by light microscopy, but lack frequent neutrophils. Some processes have disease-specific immunofluorescence findings (eg, lupus nephritis), and do not show dominant C3 or frequent hump-type deposits.