Microscopy Images
Lithium nephrotoxicity develops in patients treated long term with lithium. About 40% of patients receiving lithium may develop nephrogenic diabetes insipidus. End-stage kidney disease occurs in about 1.5% of long-term lithium users, usually after greater than 15 years of drug exposure. Patients are typically middle aged and most are white; there are no sex differences. Patients typically have low-level proteinuria, with a quarter showing nephrotic-range proteinuria. GFR loss is slowly progressive. Renal microcysts, mainly within distal tubules and collecting ducts, develop in some patients and may be seen by imaging. Patients with CKD caused by lithium nearly always also have nephrogenic diabetes insipidus.
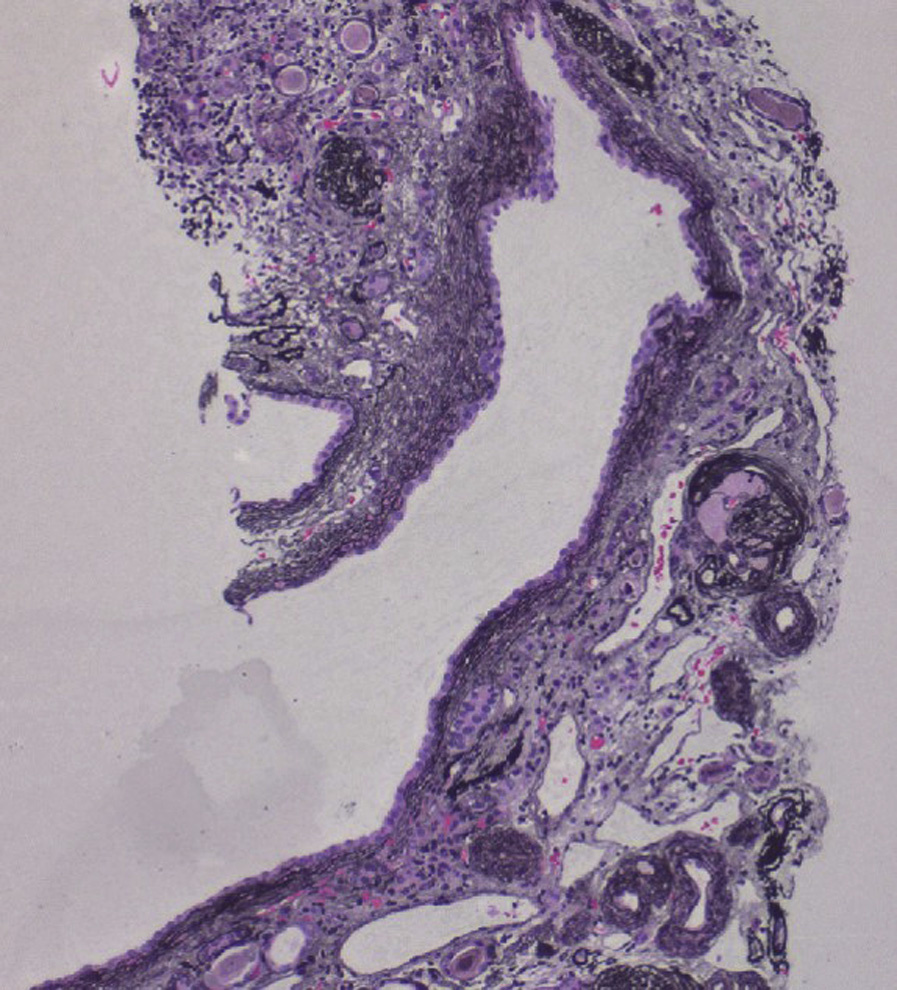
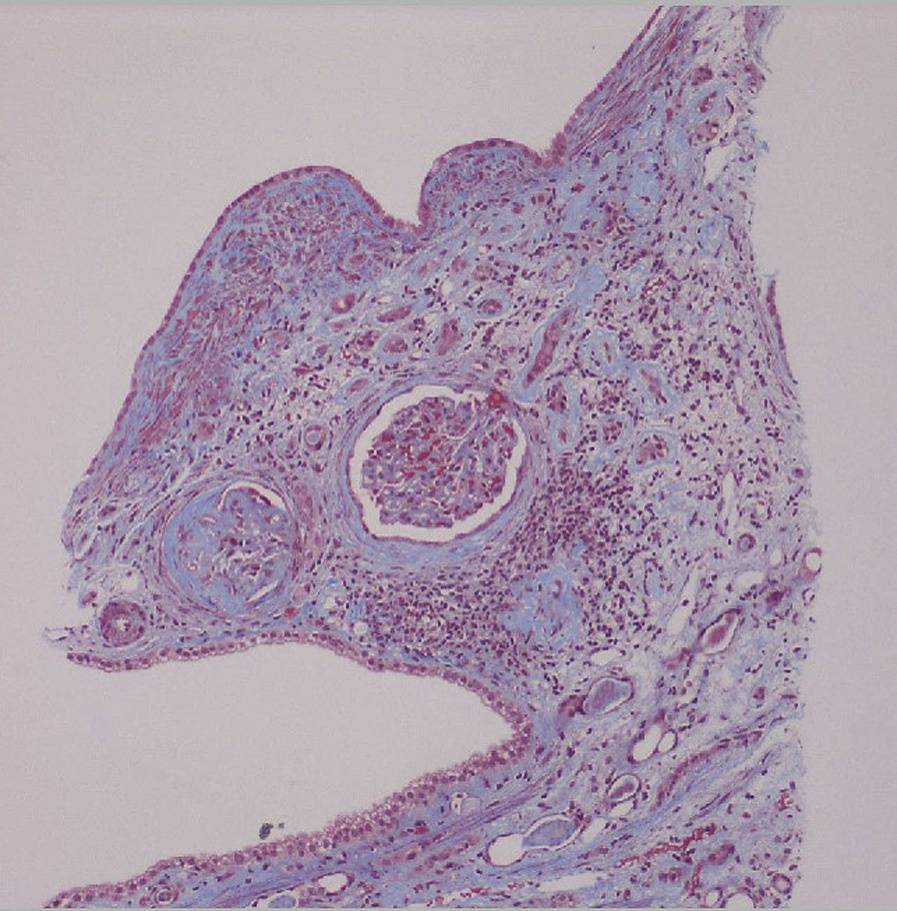
Light microscopy: Biopsies show chronic tubulointerstitial fibrosis, with possible cortical and medullary microcysts or tubular dilatation originating from distal and collecting tubules. About half of patients also have focal and segmental glomerulosclerosis and/or global glomerulosclerosis beyond that expected for the patient’s age.
Immunofluorescence microscopy: No specific findings.
Electron microscopy: There may be variable foot process effacement in the glomeruli.
Lithium causes dysregulation of aquaporin 2 (AQP2) expression, eventually leading to loss of the principal cells of the collecting duct that express these water channels and allow transcellular water reabsorption.
The epithelial sodium channel (ENaC) mediates lithium influx into these cells, where lithium inhibits glycogen synthase kinase type 3 (GSK-3) and interferes with urine-concentrating ability. The cysts commonly seen with lithium toxicity in ESRD and earlier stages of CKD are likely due to lithium uptake by the principal cells. It is postulated that nephrogenic diabetes insipidus can further enhance the pathologic effects of lithium on proximal tubules, contributing to proximal tubular atrophy and interstitial fibrosis.
Segmental glomerulosclerosis may be seen secondarily in numerous causes of CKD. When foot process effacement is extensive, the presence of cystic lesions help differentiate lithium nephrotoxicity from primary focal segmental glomerulosclerosis.