Microscopy Images
Toxic acute tubular injury describes a lesion with frank necrosis of tubules, which commonly manifests clinically as acute kidney injury, with a rapid decline in glomerular filtration rate, often oliguria, and granular casts and lowlevel proteinuria. In some settings (eg, with industrial/ environmental toxin exposures),the onset may be gradual with a slow decline in glomerular filtration rate and loss of concentrating ability. Toxic acute tubular injury may occur at any age, with varying underlying causality.
Patients may recover if the underlying etiology is recognized and ongoing injury is stopped.
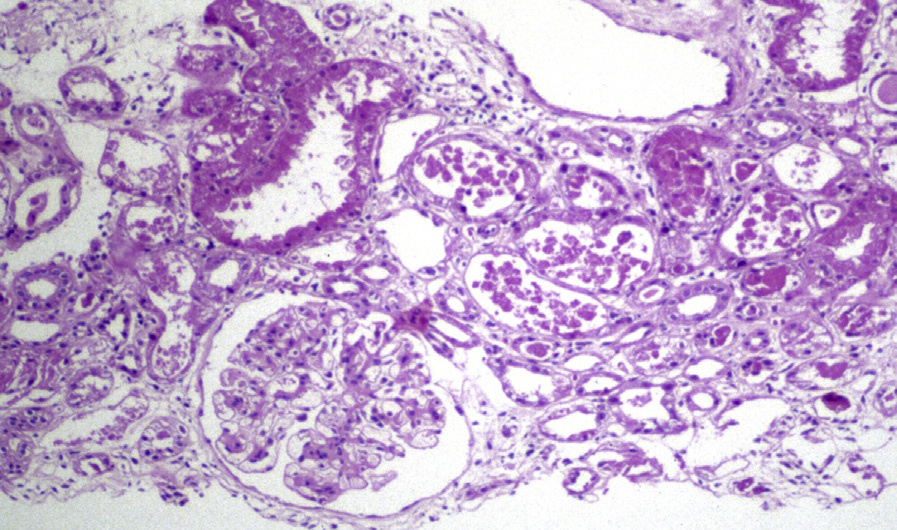
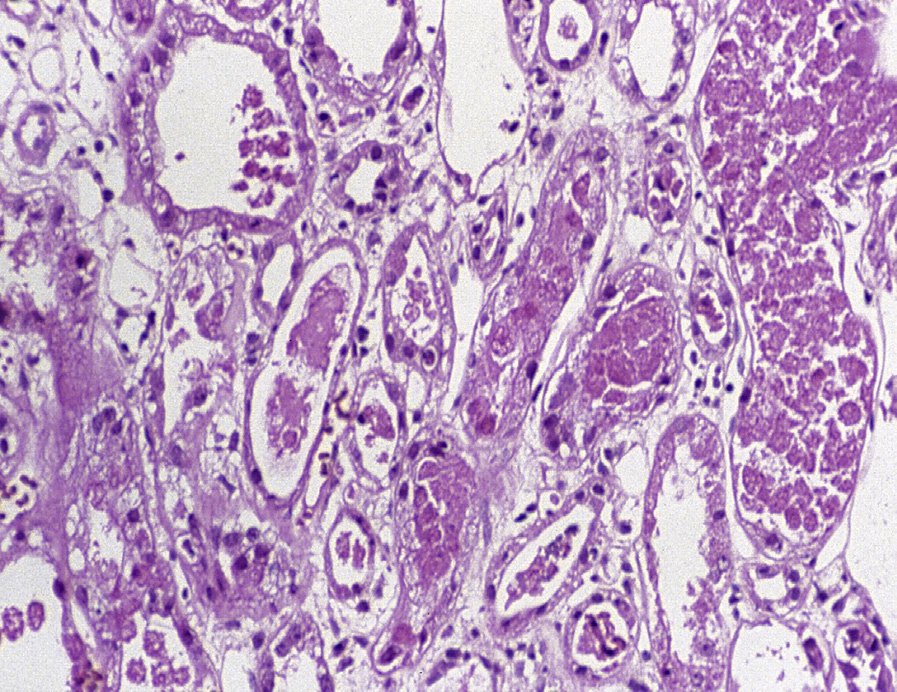
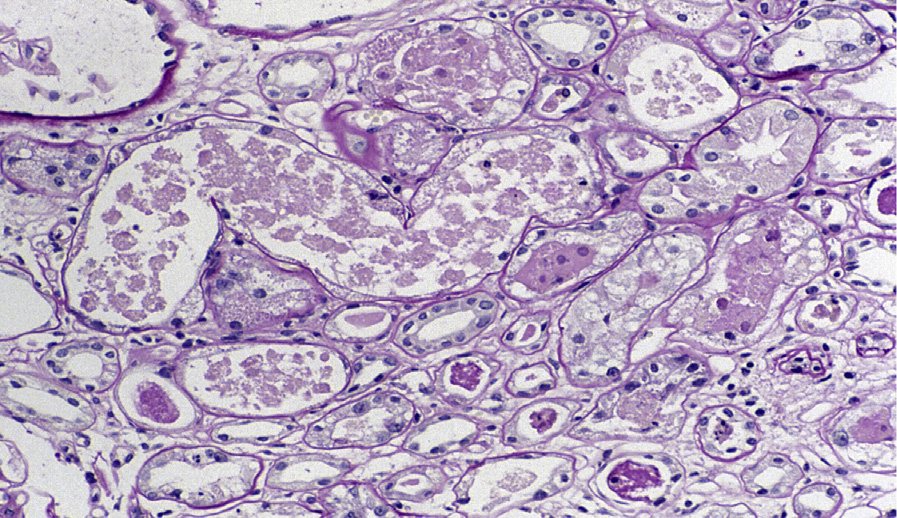
Light microscopy: Toxic acute tubular injury shows frank necrosis and sloughing of cells. Varying nephron segments are affected, depending on the toxin. The proximal tubule is most commonly and severely affected. Granular casts may be present, and tubular lumina are often filled with necrotic cells. The interstitium may show edema, but there is no significant inflammatory reaction in the acute phase, with mild interstitial inflammation as regeneration and repair ensue, with scattered lymphocytes, macrophages, and rare neutrophils and eosinophils. Reactive or regenerative changes, including prominence of nuclei and nucleoli and occasional mitotic figures, may be present in tubular epithelial cells.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: There is sloughing of tubular epithelial cells into the lumen. The injured tubular cells show loss of brush borders, apical blebs, and swollen mitochondria. Tubular cells may exhibit vacuolization and simplification of interdigitating basolateral infoldings. In aminoglycoside toxicity, there are lysosomal myeloid bodies; amiodarone toxicity shows atypical mitochondria; and lead toxicity demonstrates intranuclear lead inclusions.
Toxic acute tubular injury also can be due to medications, other exogenous substances, endogenous toxins, or crystals.
Sometimes specific morphologic features provide a clue to the underlying etiology. For example, enlarged tubular epithelial cells with abundant small cytoplasmic vacuoles are found in osmotic nephrosis. Bile, hemoglobin, and myoglobin produce distinctive casts that can be identified by specific stains; various crystals such as calcium phosphate (nephrocalcinosis), phosphate (acute phosphate nephropathy), or oxalate (primary or secondary oxalosis) have distinct appearance, and certain drugs show a characteristic electron microscopic appearance.
Specific causes of toxic acute tubular injury should be sought. Acute tubulointerstitial nephritis may have some tubular injury, but has a marked interstitial inflammatory component with tubulitis. Light chain cast nephropathy and light chain tubulopathy may be associated with significant tubular injury. Findings of specific casts, intraepithelial crystals, and immunofluorescence microscopy findings help to distinguish those entities from toxic acute tubular injury.