Microscopy Images
Patients with light chain cast nephropathy are often middle-aged or older and present with acute kidney injury. They typically have overt multiple myeloma at the time of diagnosis. Conversely, about half of patients with multiple myeloma and kidney disease have light chain cast nephropathy. There is associated nephrotic-range proteinuria, composed largely of light chains. The lesser albuminuria can manifest as lowlevel proteinuria by dipstick analysis. Patients may also have additional AL amyloid or monoclonal immunoglobulin deposition disease.
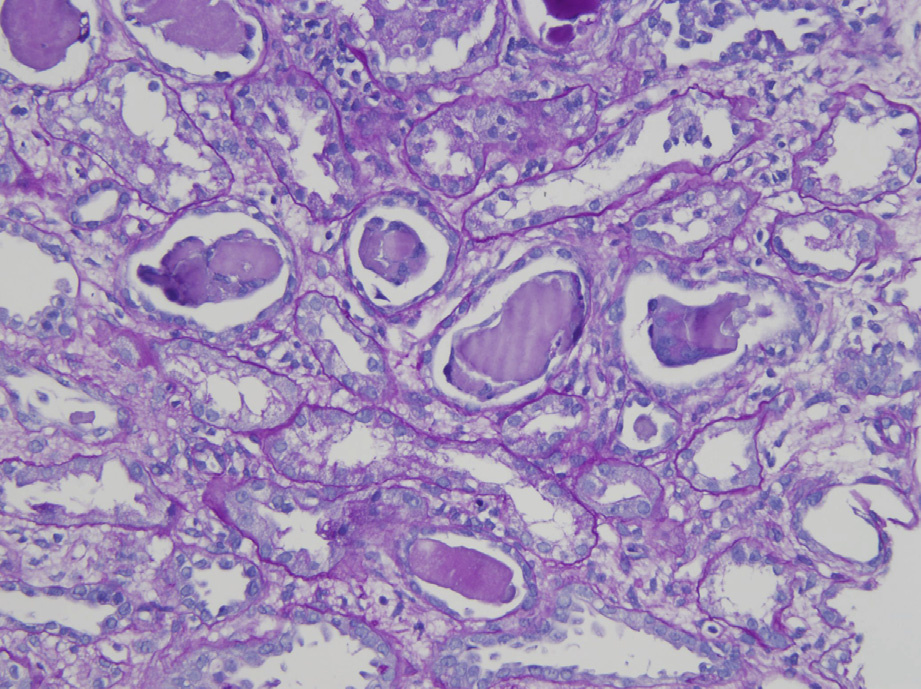
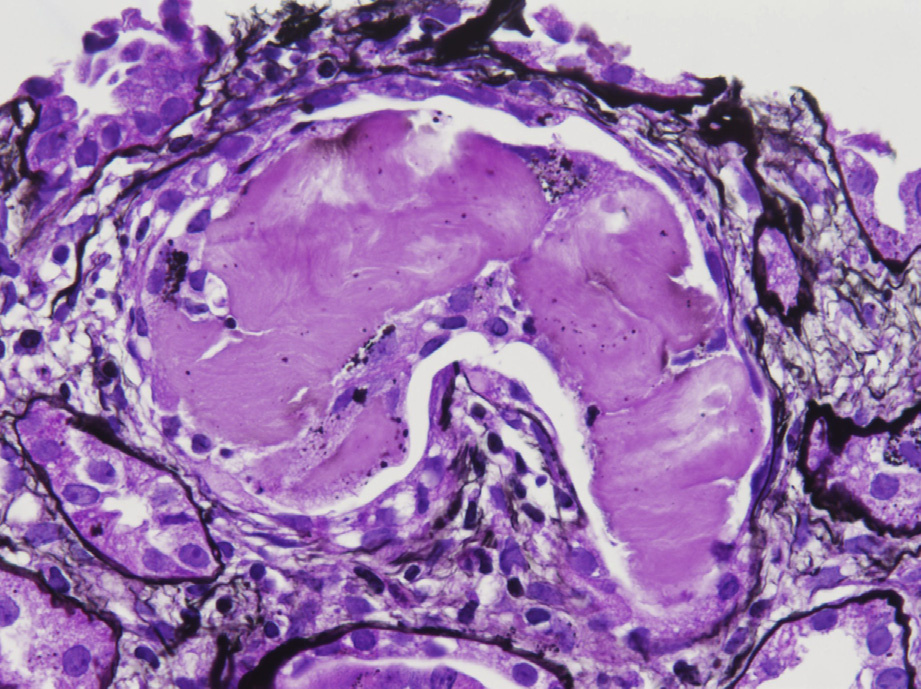
Light microscopy: The biopsy shows chronic tubulointerstitial nephritis with fractured casts that first involve the distal tubules. The casts have a metachromatic appearance due to their mixed composition of light chain (Bence-Jones) and Tamm-Horsfall (uromodulin) proteins. Surrounding cellular reaction can extend to formation of syncytial giant cells, and in the early phase may be a polymorphonuclear granulocyte reaction.
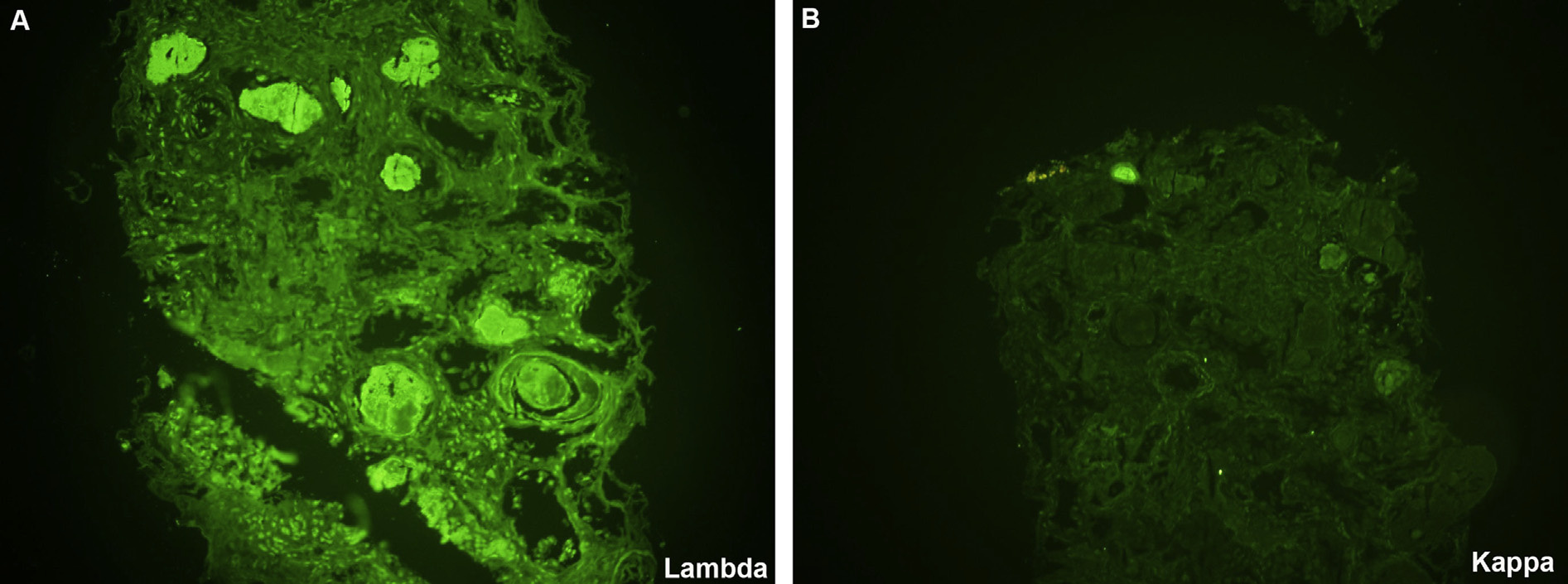
Immunofluorescence microscopy: Monoclonal staining of casts for either κ or λ light chains confirm the diagnosis, but clonal staining may be absent in some cases. Staining of formalin-fixed paraffin-embedded material after pronase digestion may unmask clonal staining in some of these cases.
Electron microscopy: Glomeruli are unremarkable, and casts show granular electron-dense material.
Crystalline substructure may be seen within these light chain casts. In rare cases, deposits of amyloid may form on the surface of the casts.
The monoclonal light chain is filtered from the glomerulus and forms casts in the distal nephron by Tamm-Horsfall (uromodulin) protein binding with the complementarity-determining region on the light chain. The casts elicit an inflammatory reaction, and may directly injure tubular cells. Furthermore, rupture of tubular basement membranes may incite a surrounding inflammatory reaction and the accompanying chronic interstitial nephritis.
Although tubules are very focally involved early on, after initial injury and cast formation, the casts may be widespread.
Light chain cast nephropathy must be distinguished from nonspecific casts and other causes of chronic interstitial nephritis, such as viral infections (viral cytopathic changes), drug-induced reactions (nonnecrotizing granulomas and tubulitis, which may have eosinophils), and tubular immune deposits (distinguished by immunofluorescence positivity along tubular basement membranes for immunoglobulin and C3).