Microscopy Images
Light chain proximal tubulopathy is due to accumulation of monotypic light chains within proximal tubules in patients with a monoclonal immunoglobulin due to low mass or smoldering multiple myeloma (about half of patients), or with monoclonal gammopathy of renal significance.
Patients commonly also have other kidney lesions related to abnormal monoclonal immunoglobulin, eg, AL amyloid or light chain deposition disease.
The proximal tubulopathy may manifest as Fanconi syndrome with aminoaciduria, phosphaturia, glycosuria in the presence of normal serum glucose, and proximal renal tubular acidosis. Patients are adults, mirroring the age in which monoclonal gammopathies and myeloma commonly become manifest. This lesion occurs in a small minority of patients in whom there is kidney disease related to monoclonal protein.
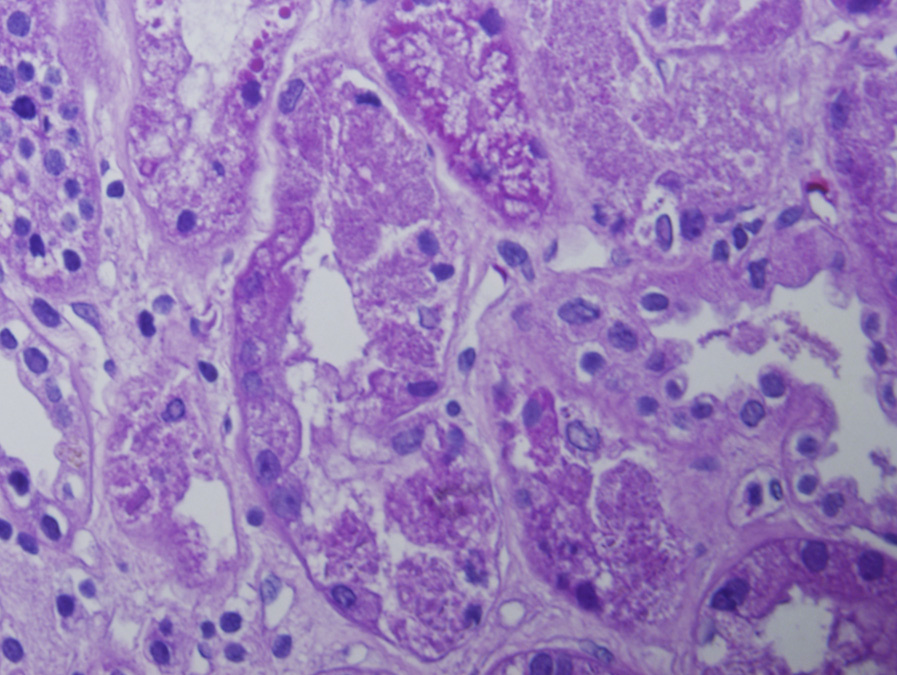
Light microscopy: Proximal tubules show loss of brush border and sloughing of tubular cells, or frank tubular necrosis. There is evidence of intratubular and intracellular crystalline inclusions or sometimes noncrystalline accumulations of light chain. Crystals are best visualized on periodic acid–Schiff and trichrome stains.
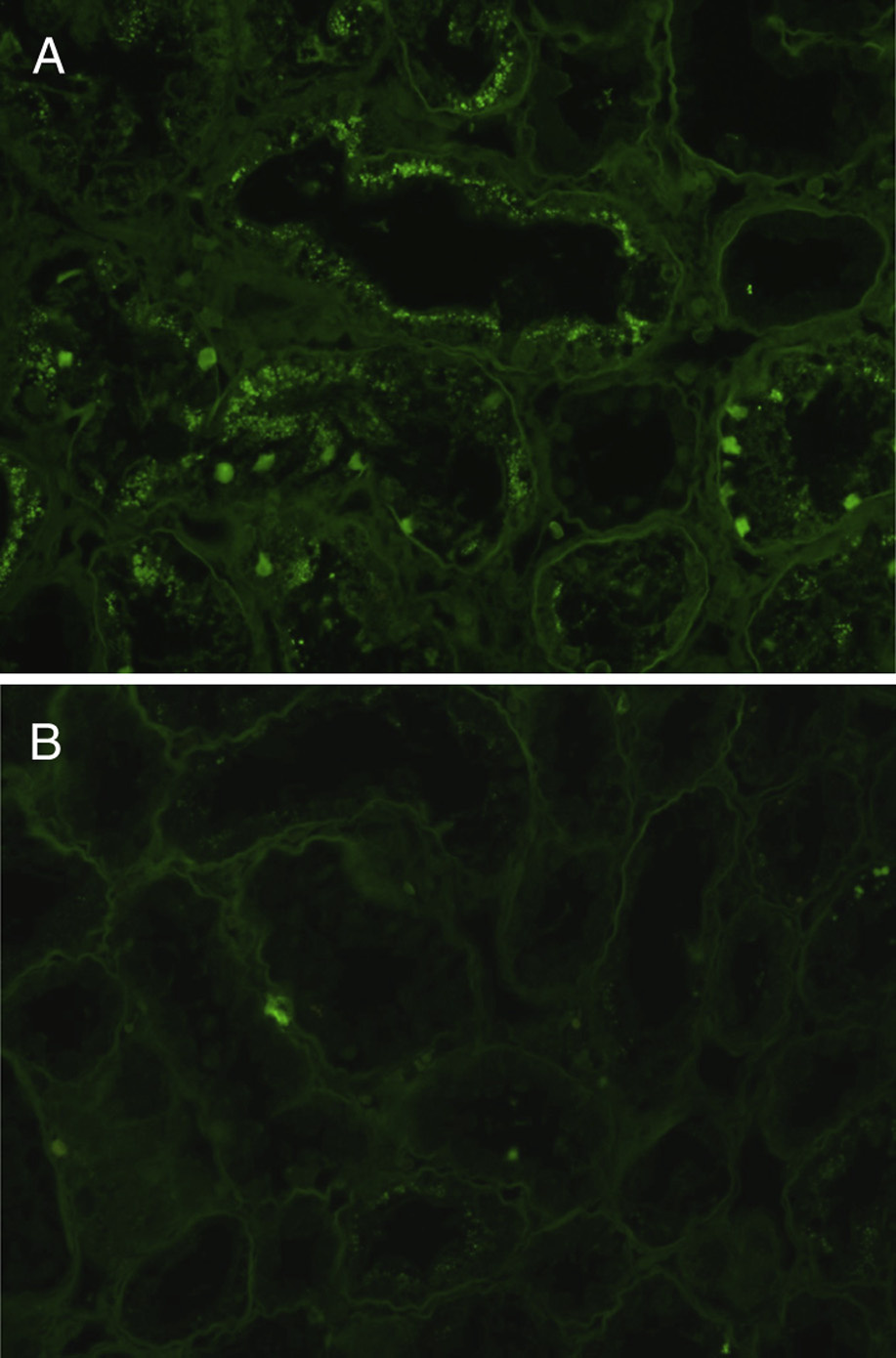
Immunofluorescence microscopy: The crystalline inclusions show monoclonal or dominant staining most commonly for κ light chain (rarely λ), which may only be detected after pronase digestion on paraffin-embedded tissues.
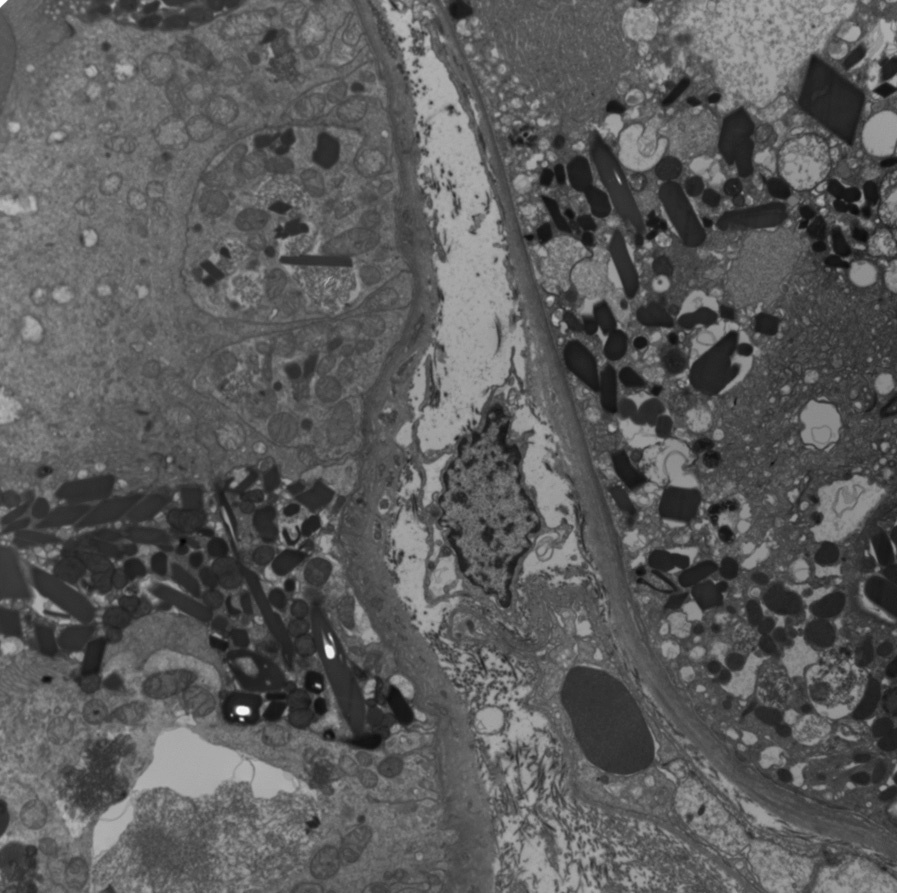
Electron microscopy: Tubular injury is evident with increased intracellular lysosomes, often containing rod-, rhomboid-, needle-, or irregular-shaped crystalline electron dense material.
Light chain proximal tubulopathy most commonly is caused by kI subgroup light chain, with inadequate lysosomal degradation of these light chains. These abnormal truncated κ light chains do not bind Tamm-Horsfall glycoprotein (uromodulin), and thus light chain cast nephropathy is not commonly associated with this lesion.
Acute tubular injury may occur from multiple causes, and demonstration of monoclonal light chains, with (or possibly without) crystalline inclusions, is necessary for specific diagnosis. Whether the noncrystalline light chain detected by immunofluorescence in proximal tubules in some patients with monoclonal gammopathy of undetermined significance represents a cause of kidney injury, or could represent physiologic tubular protein reabsorption in a patient with kidney injury from another cause, is unproven. Thus, monoclonal staining, distinct tubular injury, and decreased kidney function are necessary for suggesting this diagnosis in the absence of crystals.