Microscopy Images
Rhabdomyolysis, characterized by necrosis of muscle cells and the release of intracellular contents into the blood, is the etiology of acute kidney injury (AKI) in 7%-15% of all cases in the United States.
Conversely, 15% to over 50% of patients with rhabdomyolysis develop AKI. Rhabdomyolysis is typically characterized by muscle pain, red-to-brown urine due to myoglobinuria, and elevated muscle enzymes, including creatine kinase (CK) in the blood. The severity of symptoms varies widely, and the condition may be asymptomatic in mild cases.
Serum CK is usually at least 5 times the upper normal limit of normal, and is predominantly of the MM (skeletal muscle) fraction. It rises 2-12 hours after muscle injury and peaks in 1-3 days. Myoglobin has a shorter half-life than CK (2-3 hours) due to its rapid excretion and metabolism. Thus, CK levels may remain elevated in the absence of myoglobinuria. Urine dipstick is not specific, and turns positive for “blood” if myoglobinuria, hemoglobinuria, or hematuria is present. Higher levels of CK, volume depletion, sepsis, and acidosis increase the risk of AKI in patients with rhabdomyolysis. Most patients recover kidney function if the underlying cause can be treated, although kidney replacement therapy may be needed.
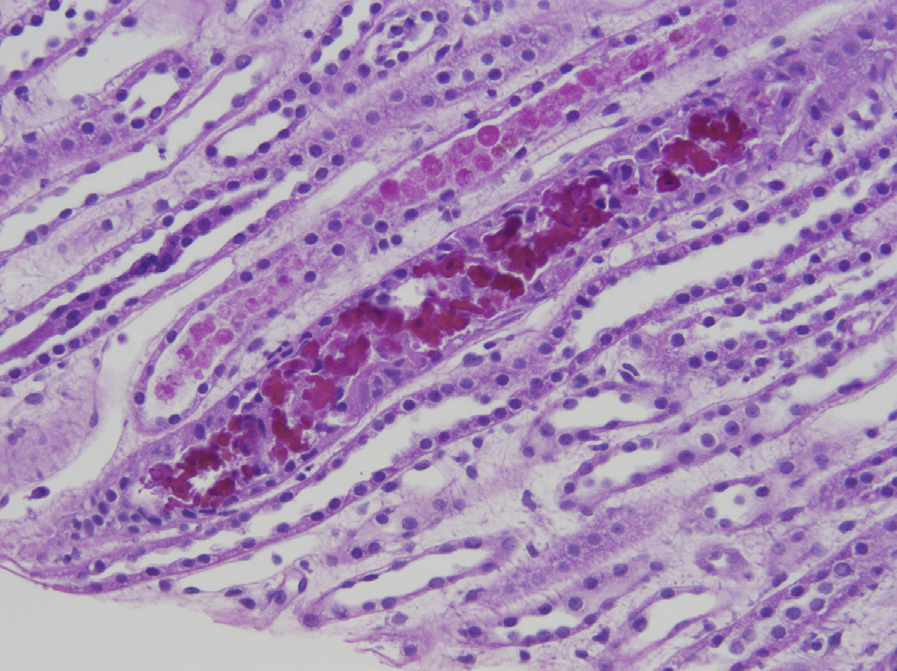
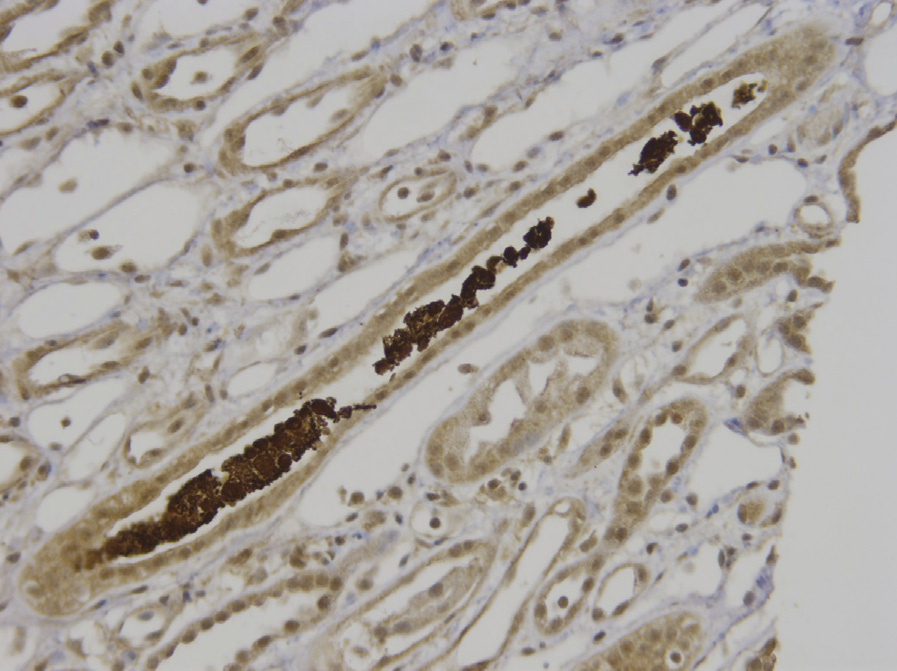
Light microscopy: There is acute tubular injury (ATI) with variable flattening of tubular epithelial cells, loss of brush borders, and intratubular sloughed epithelial cells. Myoglobin casts are composed of round granules that may line up in chains or aggregate in clusters. Their color ranges from pink to red-brown with hematoxylin and eosin stain, light brown to black with Jones methenamine silver stain, pink to bright magenta with periodic acid–Schiff stain, and bright red with trichrome stain. Immunoperoxidase staining with antibody to myoglobin is strongly positive in the casts.
Immunofluorescence microscopy: No specific staining.
Electron microscopy: Globular casts with an electron-dense core and a somewhat less-intense periphery. Substructure is absent.
Rhabdomyolysis may result from trauma, increased muscle activity (such as in severe exercise or seizure), exogenous toxins or medications (alcohol, illegal substances, cyclosporine, statins), hereditary myopathy, myositis, hypokalemia, hypophosphatemia, or hyperosmolarity. Myoglobin is filtered freely by glomeruli, then concentrated intratubular myoglobin in the presence of acidic urine precipitates with Tamm-Horsfall (uromodulin) protein to form intratubular casts that obstruct the renal tubules. Although heme pigment resulting from myoglobin degradation has a direct tubulotoxic effect, other precipitating factors such as volume depletion, acidosis, and ischemia are usually needed for myoglobinuria to induce AKI. Ferrihemate, a degradation product of heme (particularly in an acidic environment), is more tubulotoxic. Through inhibition of nitric oxide synthase, ferrihemate leads to vasoconstriction.
ATI is associated with finely granular casts, sloughed cells, and Tamm-Horsfall protein casts, which differ from the coarse granular red-brown myoglobin casts. They do not stain for myoglobin.
Light chain cast nephropathy is associated with fractured or crystalline casts with peripheral syncytial cell reaction by light microscopy, light chain bias by immunofluorescence, and a clinical history of paraproteinemia.
Hemoglobinuria-induced ATI has pigmented casts, but with clinical history of hemolysis, and casts do not stain for myoglobin. Bile cast nephropathy is associated with yellow-brown casts that appear dark green with Hall stain.
This condition occurs when serum bilirubin is very high (>20 mg/dL).